

The gallbladder stores bile produced by the liver. Our body needs this fluid to break down fats obtained from food. The fats are then broken down and absorbed in the duodenum, where the bile gets through the bile duct. Like many others, the organ can become inflamed. The condition is called cholecystitis, and if it affects the biliary tract, the name is cholangitis.
Causes of cholecystitis
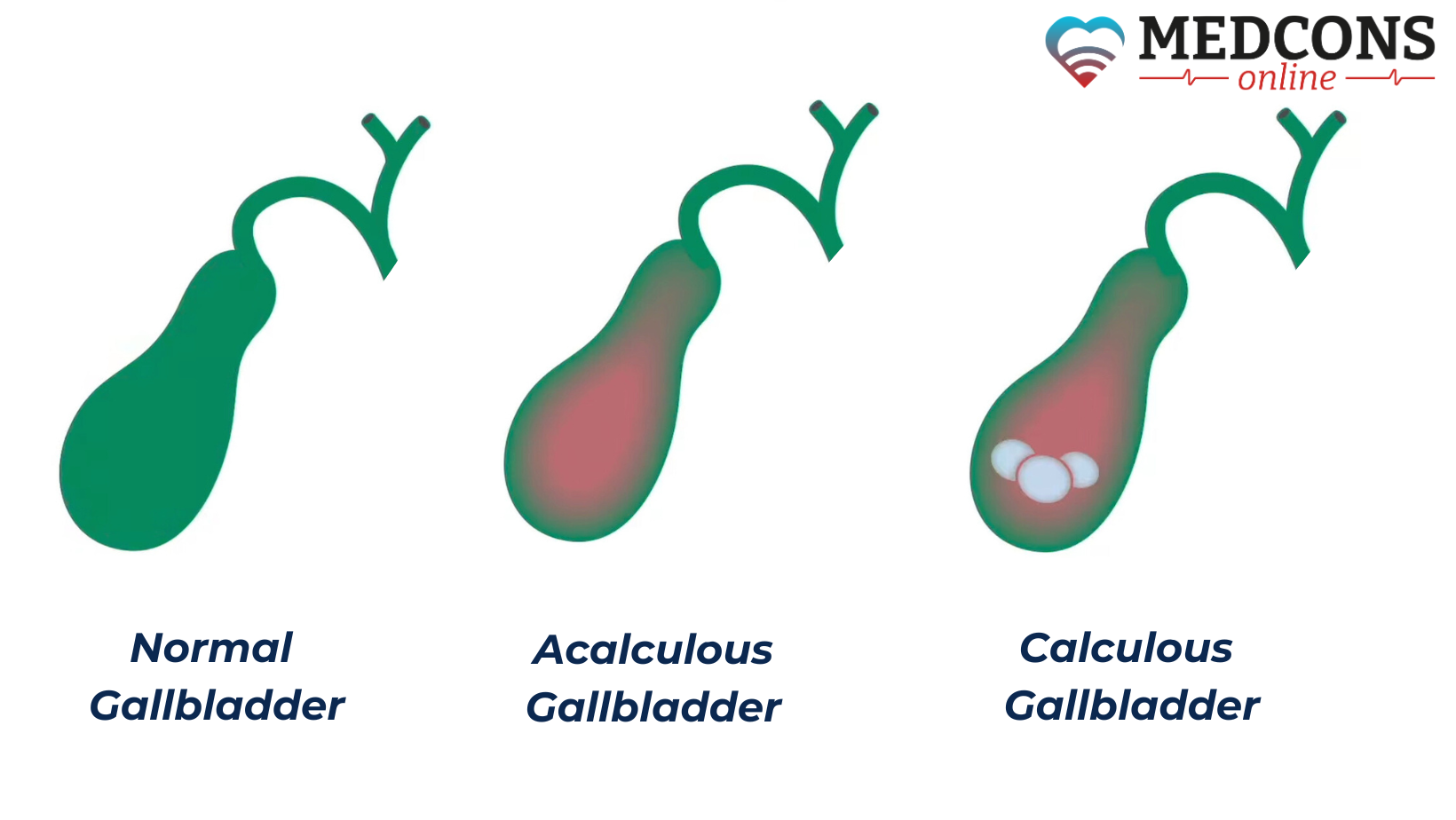
More than 90% of cases of acute cholecystitis or cholangitis are caused by gallstones, formed from hardened components of bile. They block the duct openings, making it difficult for the bile to flow into the small intestine and provoking its backflow. At the same time, bacteria that exist in large quantities in the intestine, infect the ducts and the bladder itself, causing bacterial inflammation. In addition, stones can also cause chronic cholecystitis due to constant mechanical irritation of the gallbladder wall.
Very rarely cholecystitis develops when there are no gallstones at all. For example, after severe diseases, injuries or surgeries, with acute circulatory failure or due to blood poisoning. Such a form is called non-calculous cholecystitis.
Risk factors
In general, the probability of developing the main "culprits" of cholecystitis is high. Gallstone disease affects 1 in 5-10 people in Western countries.
A common feature of many of the factors that increase the risk of cholecystitis is that the function of the gallbladder is impaired, or it cannot do its normal job at all. These include:
- Inflammation of other organs (e.g., intestines, kidneys);
- trauma (blows, accidents);
- polyps and tumors in the gallbladder;
- infections (salmonella, cholera, intestinal parasites);
- major surgical interventions in the abdominal cavity;
- prolonged starvation, artificial nutrition.
Classification
Inflammation can occur suddenly, develop slowly and over a long period of time, or relapse. Accordingly, a distinction is made between acute, chronic and recurrent forms of the disease.
In most cases, the chronic form develops from the acute one.
Besides the disease course, the presence of concretions is another classification criterion. According to it, there can be calculous and non-calculous types of cholecystitis.
Symptoms of cholecystitis
The manifestations of the disease depend on its form. They are not always specific, i.e., the same complaints can occur in other abnormal conditions.
Acute cholecystitis
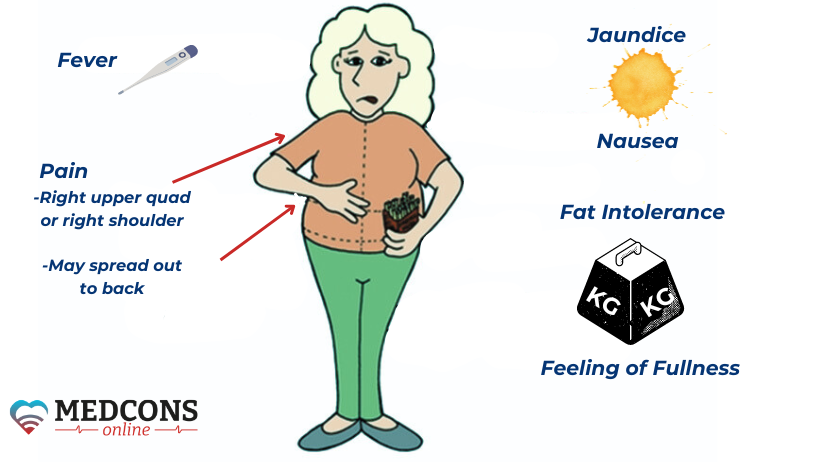
The typical symptom of acute inflammation is persistent severe pain in the right upper abdomen, often radiating to the right shoulder. They are usually accompanied by loss of appetite, nausea and vomiting, fever and chills. In the presence of stones or inflammation in the bile ducts, stool discoloration or slight jaundice may be observed. In these cases, the duct is usually completely or partially obstructed by a stone.
Chronic cholecystitis
Chronic inflammation in the gallbladder often occurs without any specific manifestations of the disease. Sometimes the symptoms are nausea or vomiting, or dull pain in the upper abdomen. Very rarely, the chronic process results in the development of the so-called "porcelain gallbladder" with a thickened, calcified wall. This condition increases the risk of cancer.
Complications
If untreated, acute cholecystitis can have life-threatening consequences, for example, in the case of gallbladder rupture (perforation). As a result, the bile flows into the abdominal cavity. This can lead to severe inflammation of the entire abdominal cavity (peritonitis). There is also a risk of affecting the liver or other neighboring organs. The infection can also spread throughout the body through the blood.
Diagnosis
The patient's anamnesis can help identify the first symptoms of inflammation in the gallbladder, or the presence of stones. This is followed by a physical examination. The doctor palpates the abdomen to determine the location and nature of pain.
The next step is usually blood tests. They can show inflammation in the body. With cholecystitis, an important indicator is an increased number of leukocytes. Other parameters indicating a pathological process are, for example, the erythrocyte sedimentation rate (ESR) and C-reactive protein. In addition, the level of the bile pigment bilirubin and some liver enzymes may be elevated in the blood.
Imaging is also used to diagnose cholecystitis. In most cases, gallbladder inflammation can be detected with a simple ultrasound scan. If necessary, additional diagnostic procedures are performed. These include endosonography, computed tomography or magnetic resonance cholangiopancreatography (MRCP).
Another diagnostic method is endoscopic retrograde cholangiopancreatography (ERCP). In this study, the doctor inserts a flexible instrument (endoscope) in the form of a tube through the mouth, oesophagus and stomach into the small intestine. There, a contrast agent is injected into the bile duct, and an X-ray is taken. During the examination, gallstones can be immediately removed from the ducts with the help of an endoscope, which makes it a therapeutic procedure.
Treatment of cholecystitis
Therapeutic strategy mainly depends on the cause and severity of cholecystitis. Surgical removal of the gallbladder (cholecystectomy) is usually indicated in the case of acute inflammation. Depending on the symptoms, antibiotics are also administered, e.g., if there are signs of complications such as abscess or sepsis.
Conservative treatment
Dissolution of stones with ursodeoxycholic acid preparations is considered as an option only in selected cases, in symptomatic patients with small concretions presumably consisting of cholesterol.
In acute cholecystitis with signs of sepsis, cholangitis, abscess or perforation, antibiotics are given immediately.
Surgery
The gallbladder is usually removed by laparoscopic surgery. The instruments needed for the operation are inserted into the abdomen through several incisions only a few millimetres long. This is a much gentler method than open surgery. Only very small scars are left, and recovery is very quick.
Only in rare cases - e.g. in case of large stones, advanced inflammation or complications - is it necessary to open the abdominal wall through a larger incision.
Prognosis and prevention
The absence of a bile reservoir does not usually cause significant problems, as it continues to be produced in the liver and goes straight into the small intestine. After surgery, there is absolutely no need to make changes to the usual meal plan or to follow a special diet.
To prevent cholecystitis, attention should be paid to reducing individual risk factors. Lifestyle changes including physical activity and an appropriate diet can prevent the formation of cholesterol gallstones.
Conclusions
Knowing the mechanisms of occurrence and risk factors of cholecystitis, its development can in many cases be prevented. To keep the disease from entering an acute stage, and avoid unexpected attacks, one should not ignore troublesome symptoms occurring after meals. If the diagnosis has already been made, you should not rely on folk remedies to dissolve gallstones, or hope that it will pass by itself. To cure the disease, a qualified doctor should be seen without delay (a remote appointment can do as well). This will provide a prompt and effective solution of the issue.
References
- S3-Leitlinie zur Prävention, Diagnostik und Behandlung von Gallensteinen, AWMF-Register-Nr. 021/008. Empfehlung IIIB.8. AVMF, 2018, S. 930, abgerufen am 20. Oktober 2020.
- Collins, Edwards (2013). A Short Course in Medical Terminology. Lippincott Williams & Wilkins. p. 246. ISBN 9781469835785. Archived from the original on 2017-09-08.
- "Cholecystitis". The Lecturio Medical Concept Library. Retrieved 8 July 2021.
- "Acute Cholangitis". The Lecturio Medical Concept Library. Retrieved 27 June 2021.
Comments — 0