

The need for a heart valve procedure occurs when it fails to cope with its function due to various circumstances. In such cases, cardiac surgeons come to the rescue.
Why do some patients have to undergo heart valve surgery?
Acquired, i.e., developing during the lifetime, heart valve diseases can occur for a variety of reasons. In addition to wear and tear, the valves often suffer from other factors, such as calcification (sclerosis), cholesterol deposits, bacterial inflammation, rheumatic fever, heart attack, etc. In addition, there is a large group of congenital valve disorders.
The abnormality consists in the incorrect blood flow between the heart chambers and, consequently, the release of blood into the general circulatory system.
When there is a significant narrowing of the opening between the heart chambers, for example, due to sclerosis, doctors speak about stenosis. If the valve fails to close the opening between the chambers properly (which can be caused not only by the organ itself, but also by various reasons related to changes in the size of the heart chambers), we are dealing with valve failure (regurgitation).
Both issues gradually lead to significant abnormal changes in blood flow, heart muscle overload, and its gradual weakening.
At first, these developments may remain imperceptible, causing no obvious symptoms. But over time, the heart becomes so overstressed that it ceases to cope with its work. The weakening of its muscle is life-threatening. The medications that support it become less and less effective. Thus, one is confronted by a situation where the only solution is heart surgery – either the reconstruction or replacement of the diseased valve.
What procedures can be used to treat heart valve disorders?
If surgery becomes unavoidable, cardiac surgeons first decide whether the organ can be preserved by "repairing" it, or whether it must be removed and an artificial one implanted instead.
In the latter case there is the issue of choosing the type of prosthesis. Basically, there are two types - mechanical or biological. The decision is always made collectively by cardiologists, cardiac surgeons and anesthesiologists together with the patient, with whom the pros and cons are discussed.
How are artificial heart valves created, and what types are there?
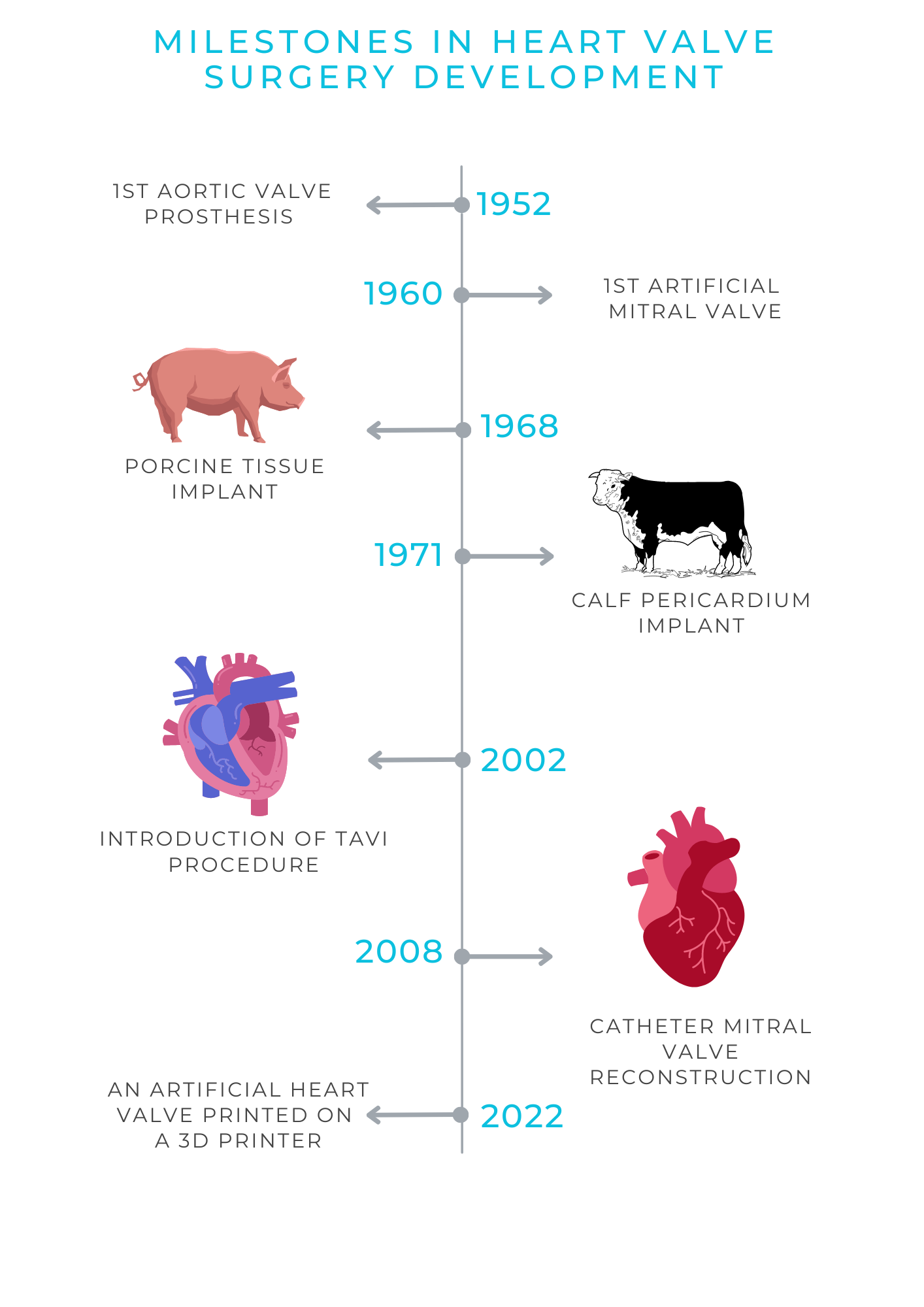
The history of prosthetic heart valves dates back to 1952, when US surgeon Charles Hufnagel first implanted an artificial aortic valve in a severely ill 30-year-old woman. The patient survived and returned to normal life.
Since then, valve surgery has progressed steadily. Doctors, engineers, chemists, and other specialists have continually improved surgical techniques and the materials used to make prostheses.
Today, valve replacement has become quite a routine procedure at specialized cardiac surgery facilities.
Various implant modifications have allowed hundreds of thousands of people to return to a full life. Inventors have already developed more than 80 models made of metal, synthetic composites, textiles or animal tissues; with wings, caged balls and flaps. All of them present a combination of high technology and handiwork. Each such prosthesis is a small technical marvel.
Just like real valves, the prostheses allow blood to flow only in the intended direction - either inside both ventricles or out again. Between two heart beats, they close, which prevents backflow of blood.
Mechanical prostheses are made entirely of artificial materials. To ensure a "non-return" function (i.e., to prevent backflow), the so-called bileaflet design is most often used. Two semi-circular flaps, attached to a rigid ring, swing open and close, like the doors of cowboy saloons in the Wild West movies. The flaps and ring are made of synthetic material, mostly extremely strong pyrolytic carbon, and framed by a polyester cuff.
Under special conditions and using a microscope, it is sewn onto a wire frame by hand. In the production process, the tissue is first chemically treated in order to prolong the viability of the prosthesis and prevent host reaction.
In 2022, scientists at the University of Munich produced a heart valve on a three-dimensional printer. For this purpose, an advanced additive (i.e., creating an object from an electronic model) technology called "melt electrowriting" (MEW) was used. It is expected that in the future prostheses will be created in this way, growing with the body, so they can also be used in children.
Advantages and disadvantages of mechanical and biological prostheses
A huge advantage of mechanical heart valves is their durability. They last practically for life. The likelihood that the flap will break is extremely low, occurring in about one in 10,000 patients. But the disadvantage is the favorable conditions for thrombus formation on the surface of the prosthesis. Therefore, a lifelong administration of blood thinning medications is necessary to prevent thrombus formation.
It is also known that every sixth patient with an artificial valve feels a metallic clicking sound when it slams shut.
This is not the case with biological prostheses. In their case, anticoagulants are needed only temporarily. Later only low doses of aspirin are sufficient.
However, implants made of animal tissue have a relatively short lifespan. After 10 to 15 years, the prosthesis calcifies or undergoes a natural wear and tear process, so that it must be replaced.
Among other things, this is also due to the fact that the heart works under greater strain in the young. Therefore, durable mechanical implants are preferable for patients younger than 65 years of age, and after 65 biological implants that do not require constant blood thinning are better.
How is reconstruction performed?
In the case of aortic regurgitation, the valve is usually reconstructed by minimally invasive method through cutting only the upper third of the sternum. The "repair" type itself depends on the underlying disease that led to the insufficiency. In many cases normal function is restored by reducing the ring and reconstructing the cusps. In cases of aortic aneurysm, it is replaced by a vascular prosthesis made of artificial material, in which the own aortic valve is sewn.
Reconstruction of the insufficient mitral valve, as a rule, is performed also in a minimally invasive way (minimally invasive thoracotomy). The procedure is performed through the intercostal space without damaging the sternum. The treatment usually includes fibrous valve ring annuloplasty and replacement of torn tissues.
In patients with dilated left heart chamber, innovative surgical techniques based on changing the geometry of the heart chamber are used today.
Tricuspid valve reconstruction is also a minimally invasive procedure. The most common cause of its leakage is right atrial enlargement. In most cases, repair is limited to ring annuloplasty.
What are the ways in which heart valve interventions are performed?
The gold standard of operations involving artificial valve implantation or valve reconstruction is open surgery.
At the same time, modern cardiac surgery very often uses minimally invasive techniques with a partial incision of the upper part of the sternum. This method allows to sustain chest stability, and has a good cosmetic result. The surgery is performed using a heart-lung machine. The conventional method is still very common due to the very good long-term results and low surgical risks.
However, a 2-3-hour operation under general anesthesia can only be tolerated by patients who are strong enough. In 2002, doctors found an alternative. The procedure is called TAVI (transcatheter aortic valve implantation). The procedure is performed under local anesthesia. The surgeon "advances" the folded artificial valve into the heart through the groin artery. The diseased valve remains in the body, it is simply moved sideways with the implant.
Thus, in 2019 as many as about 60% of all aortic valve replacements were performed via catheter. However, it must be taken into account that the new valve can put pressure on the conduction pathways that determine the heart rhythm, so about 10% of those who underwent this operation later need an artificial cardiac pacemaker installed. With the conventional technique, this figure is half as much. Strokes are also somewhat more common after TAVI, although overall those are very rare.
Since 2008, catheter procedures have also been used in mitral valve treatment. The most common of these is currently MitraClip, it has been performed in more than 100,000 patients worldwide. The MitraClip is the patented name of a clip device that is delivered to the heart via a flexible tube (catheter) inserted through the inguinal vein. There, the clip attaches to the two valve flaps, locking them in an optimal position. Thus, regurgitation is stopped. In 2019, an improved modification of this operation, the PASCAL technique, was introduced. Later came the Cardioband, which is performed according to the same algorithm, but to restore tightness in this case an implant (a ring attached to the fibrous ring of the mitral valve) is installed.
In certain cases of aortic valve replacement, e.g., in very young patients for whom the continuous administration of blood thinning medications is undesirable or impossible (e.g., women who still want to have children), the so-called Ross operation is used. The patient’s own pulmonary valve is used as replacement, and a donor valve (homograft) is placed instead of it. This is a good option for young patients preferring an active lifestyle.
Finding the best solution together
It is not always easy and quick to determine which procedure and implant type is the best in each individual case. Therefore, such decisions are always made jointly by cardiac surgeons, cardiologists, and anesthesiologists. If necessary, other specialists also get involved.
To obtain such an assessment one does not to undergo all exams once again. As a rule, the available findings and reports are sufficient to get a second opinion and make the final decision.
References
- Echte Handarbeit. FOCUS Gesundheit Nr.93 – Herz & Kreislauf. ISSN 2199-5087
- Filippo Calì MD, Matteo Pagnesi MD, Elisa Pezzola MD, Andrea Montisci MD, Marco Metra MD, Marianna Adamo MD. Transcatheter edge-to-edge mitral valve repair for post-myocardial infarction papillary muscle rupture and acute heart failure: A systematic review. Wiley Online Library, 10 May 2023. | https://doi.org/10.1002/ccd.30682
- Totally endoscopic aortic valve replacement: Techniques and early results. Front. Cardiovasc. Med., 09 January 2023. Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1106845
Comments — 0