


Generous and fatty meals may sometimes provoke sudden cramps and severe pain in the right upper abdomen. If a piece of creamy cake or a few hard-boiled eggs lead to such unpleasant consequences, most likely, you should suspect gallstone disease.
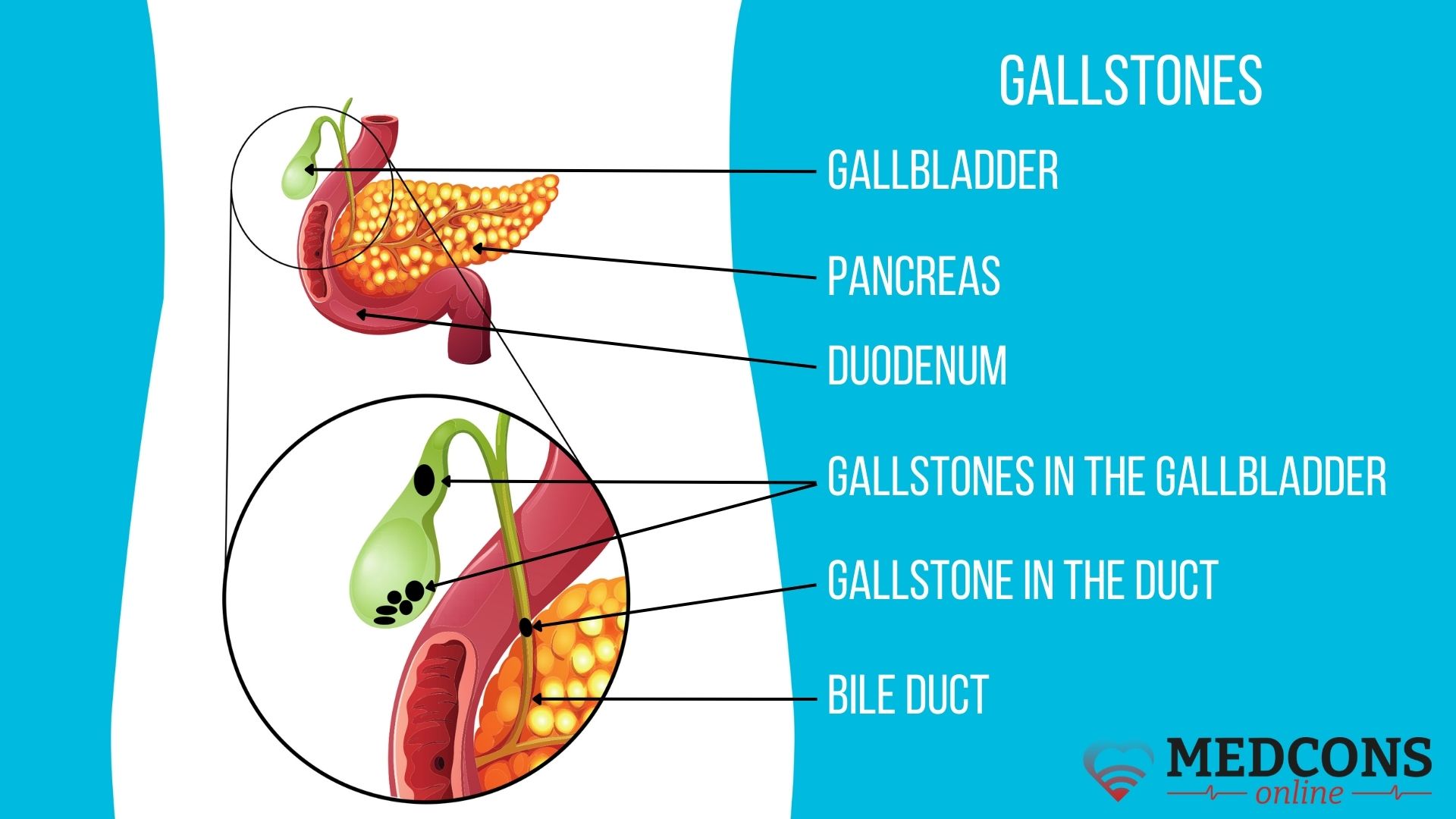
Its core is the presence of one or more stones in the gallbladder. Having reached a certain size, they block the ducts that transport bile to the duodenum. The muscles surrounding the gallbladder try their best to remove the obstacle with the help of contractions. If this fails to bring immediate success, a pain syndrome develops.
Definition of the disease. Causes of the disorder
Gallstones are accumulations of crystals in the gallbladder or bile ducts, which may have different compositions. These can be the cause of gallstone disease (the medical term is cholelithiasis).
The occurrence of cholesterol crystals, one of the possible stone types, is associated with changes in bile composition. In normal bile, acids and cholesterol are in a certain ratio. Acids ensure that water-insoluble cholesterol is kept dissolved. If the liver secretes too much of this substance, or the bile acids are low, the bile becomes saturated with cholesterol to form crystals. They join together, gradually building a light-yellow lump.
The formation of another type called pigment stones is caused by the production of large amounts of bilirubin (yellow blood pigment). In this case, the normal process of its transformation into soluble breakdown products, or their excretion, is disturbed. This can occur due to severe liver diseases, such as cirrhosis, as well as in infections.
Usually, concrements start to build up in the gallbladder, less often (5-10%) in the bile ducts. They frequently remain unnoticed at all, but in about 25% of cases can lead to an attack of sharp pain in the right subcostal region. This condition is called biliary (or hepatic) colic. It occurs when a crystal formation enters the common bile duct or any of the other biliary tracts and blocks it, which favors bacterial growth and can lead to bacterial infections. As a result, a scar obstruction develops, making it difficult to drain bile even after the stone has passed.
Gallstones risk factors
Women are known to be much more susceptible to the disease than men. The female sex hormone oestrogen is thought to contribute to the development of stones. Therefore, in particular, the risk is increased in women taking hormone replacement therapy. Other risk factors are obesity and age (40+).
The disease can also be associated with severe weight loss and some weight loss procedures (bariatric surgery). The likelihood of getting the disease is significantly increased after gastric bypass surgery.
In addition, genetic predisposition also plays a role.
Over the course of a lifetime, such people are 2-3 times more likely to develop gallstones than others. The gene contains the scheme of a molecular "pump" that transports cholesterol from liver cells to the bile ducts. Genetic modification, apparently, makes this pump constantly work at full capacity.
Symptoms of cholelithiasis
The first disease manifestations can sometimes be very non-specific and resemble symptoms of other diseases. If eating fatty food results in a feeling of fullness and pressure in the upper abdomen, accompanied by heartburn or flatulence, this may indicate the presence of gallstones. Sometimes the patient suddenly becomes intolerable to certain foods, for example, coffee.
When the biliary tract gets blocked, the pressure in the gallbladder/bile duct system increases, which leads to an attack (the so-called colic). Its characteristic features are sharp, wavy pain localized in the middle or right upper abdomen, sometimes spreading to the back and up to the shoulder blade. In some cases, it is accompanied by vomiting. Its intensity rapidly increases, then reaches a "plateau" and decreases sharply (spontaneously or after drug therapy). The duration of this condition is usually from 15 minutes to several hours. It occurs predominantly at night and often does not coincide with meals. Most patients remember the pain onset very accurately.
Gallstone disease classification and stages
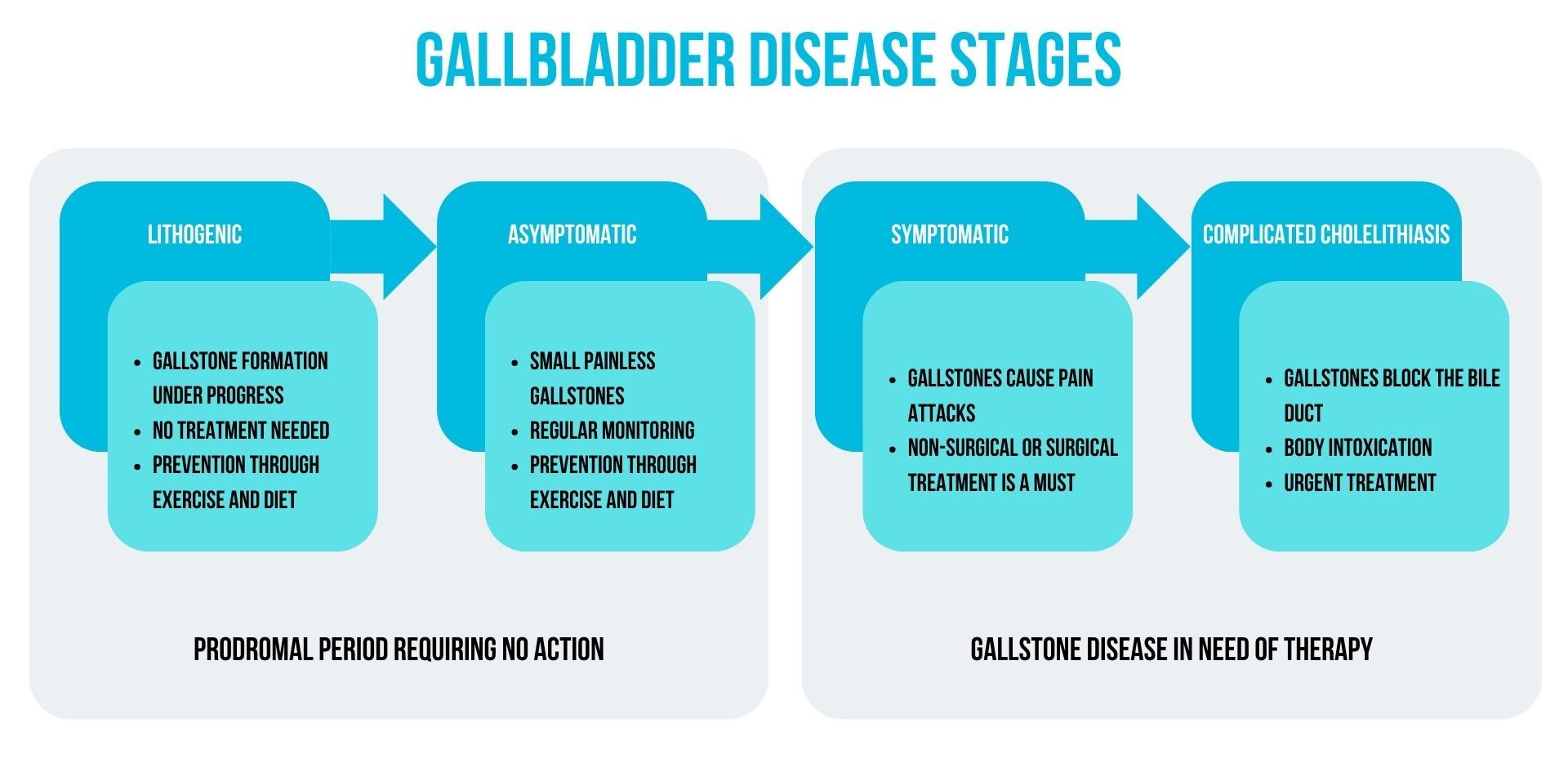
The cholelithiasis classification distinguishes four stages, which influence the treatment strategy.
I. Lithogenic
This condition can be called "pre-gallstone disease". At this stage, there are already conditions in the gallbladder that can lead to the formation of lumps, but this has not yet happened. Therefore, the disease can still be prevented; however, no treatment is required. Exercise and a healthy diet with limited fat intake, plenty of leafy vegetables, whole-grain products, legumes and fruit can help.
II. Asymptomatic stones
Stones have already formed, but they are small and are excreted by themselves without causing blockage of the bile ducts. There are no symptoms, and the crystals are only discovered incidentally if an examination is carried out to prevent or diagnose another disease. Treatment is still not necessary. The management strategy in this situation is to get enough physical activity and follow a healthy diet. Regular monitoring is necessary not to miss the moment when the condition progresses to a more severe stage.
III. Symptomatic stones
The patient manifests attacks of abdominal pain, especially after eating. This condition is already definitely a disease. It is necessary to see a doctor immediately to plan further action (conservative treatment or intervention).
IV. Complicated cholelithiasis
The last stage of LCB development is a serious and potentially dangerous condition, when nausea, vomiting, indigestion, abdominal bloating add to the pain. Treatment is mandatory, and the question of surgery arises.
Complications of cholelithiasis
If a stone blocks the gallbladder duct for more than a few hours, acute inflammation of the gallbladder (cholecystitis) may develop. Later on, suppuration (empyema) and even perforation of the gallbladder wall may occur. All this threatens with peritonitis.
If the lump completely blocks the common bile duct, bile does not enter the small intestine and gets accumulated. This leads to jaundice and darkening of the urine; the stools become pale, the skin and eyeball turn yellow. Due to bile stagnation, bile duct inflammation (cholangitis) begins. Later, in addition to attacks of pain in the upper abdomen, fever and chills appear (Charcot's triad). In addition, obstruction in the bile papilla area leads to inflammation of the pancreas (biliary pancreatitis).
As a result of mechanical irritation alone, its wall calcifies and becomes inelastic. Calcium makes it clearly visible on X-ray (the so-called "porcelain gallbladder"). By losing elasticity, the organ can no longer contract fully, and therefore cannot fulfil its function. This condition is relatively rare, but is associated the risk of cholangiocarcinoma.
Diagnosis of the disease
If cholelithiasis is suspected, a comprehensive examination by a general practitioner or gastroenterologist is carried out. An integral part of it is ultrasound examination. Depending on the nature of complaints, other diagnostic procedures are also used.
Examination and history taking
Careful collection of information about the nature and timing of complaints, as well as a specific clinical examination, helps to determine the course of further action. In particular, at this stage the doctor:
- Shall assess the general physical condition (blood pressure, pulse, weight, condition of the skin, mucosa and sclerae).
- Shall proceed with percussion (tapping) and palpation of the abdomen to detect ascites, flatulence, liver enlargement, Murphy's sign (pain on deep breath), as well as to differentiate the condition (from appendicitis, peptic ulcer, functional dyspepsia, gastric infections).
Lab tests
With the help of blood tests, the doctor detects various abnormal changes characteristic of gallstone disease.
| Abnormal condition | Indications |
| Acute inflammation | ↑ ESR, C-reactive protein, leucocytes |
| Bile outflow disorder | ↑ Bilirubin |
| Liver damage | ↑ Transaminase concentration (ALT, AST) |
Gallbladder ultrasound
Sonography is a standard procedure for diagnosing stones and other issues in the gallbladder.
Ultrasound scans also show an increase in the size of the bladder and thickening of its wall associated with fluid accumulation (oedema), which are typical signs of inflammation. The procedure can also detect bile duct dilation.
Computed tomography or magnetic resonance imaging
CT or MRI can be useful in the case of complications, such as perforation and bile duct stones, or to rule out tumors. However, they are mostly unnecessary in the detection of gallstones and acute cholecystitis.
Endoscopic retrograde cholangiography (ERCP)
This technique is an endoscopic examination of the bile ducts performed retrogradely (i.e., through the stomach and duodenum) with the injection of a contrast agent. It enables not only visual inspection, but also therapy, such as dilating the lumen from the bile duct into the duodenum (papillotomy), or placing a stent.
Magnetic resonance cholangiopancreatography (MRCP)
MRI protocols can be specifically adapted to better display the liver, biliary tract and pancreas. This is called MR cholangiopancreatography. It is a non-invasive alternative to ERCP.
Endosonography
Endoscopic ultrasound (endosonography) is performed to find out why the bile flow is disturbed. As with gastroscopy, a special endoscope is inserted into the duodenum. There, with the help of ultrasound, the condition of nearby tissues is assessed. In special cases, the doctor may take tissue samples under ultrasound control for microscopic evaluation.
Cholelithiasis treatment
An intervention is needed only if there are specific symptoms. In other cases, conservative management of the disease is appropriate.
Surgery
In uncomplicated cases of gallstones accompanied by specific pain, removal of the gallbladder (cholecystectomy) is indicated. Its objectives are to:
- to eliminate the causes of pain;
- to prevent the development of gallstone complications or to reduce the existing ones;
- rule out the possibility of developing gallbladder carcinoma in high-risk patients.
Two types of surgery are generally possible:
Open surgery: removal of the organ under general anesthesia through an incision in the abdominal wall (most often under the right rib arch). Currently, this method is used very rarely; for example, if a tumor is suspected, if there are extensive adhesions, or when inflammation spreads beyond the gallbladder wall.
Laparoscopy: the gallbladder is removed "through a keyhole". The surgeon inserts a camera and working instruments through three small incisions in the abdomen. The advantage of this method over open surgery is the absence of a large surgical wound in the abdomen. This reduces the risk of complications, lessens postoperative pain and speeds up recovery.
If stones are found in the biliary tract as well, cholecystectomy can be combined with removal of lumps from the duct with the help of ERCP.
Rehabilitation
The patient must refrain from eating and drinking for the first four hours after the operation. After that, you can eat normal food, but it is recommended to avoid too fatty foods at first. Subsequently, no special diet is necessary; you can eat everything (of course, within reason).
For some time after cholecystectomy there are pains, but they are easily relieved with medication. On the second day following the procedure, the doctors check laboratory parameters and make an ultrasound scan of the surgery area. If laparoscopy was performed, the patient is usually discharged shortly afterwards. In the case of open surgery, hospital stay lasts a little longer.
Within one or two weeks after leaving the hospital, it is recommended to refrain from normal physical activity. It is not allowed to lift weights of more than 5 kilograms for 3-4 weeks.
Prognosis
If the stones have already manifested themselves, the risk of biliary colic recurrence is very high.
After removal, the probability of complications is significantly reduced. The operation is successful in 80-90% of patients, acute symptoms no longer occur, but some may still experience digestive problems afterwards. In rare cases, bleeding or damage to other organs may occur during the intervention.
Dissolution of gallstones
If the bladder neck is not blocked, cholesterol masses can in principle be dissolved with a drug containing ursodeoxycholic acid. When taken two or three times a day, it can dissolve small formations within 6 months. However, such treatment is not considered as a full-fledged alternative to surgery by modern medicine. First, the effect is possible only in the case of really small crystals. Second, in about half of the patients, stones form again within five years after successful dissolution.
Prevention
Drug prophylaxis of cholelithiasis is not usually prescribed. However, if the risk of stone formation is high, ursodeoxycholic acid can be administered for a limited period of time.
In particular, it can be prescribed to young patients with primary diagnosed or recurrent disease, and a confirmed ABCB4 gene mutation, leading to chronic cholangiopathy and contributing to the formation of cholesterol gallstones.
Gallstones diet
No diet is capable of dissolving the stones as soon as they have already formed, only medicines can do it.
If you have or are known to be at risk of gallstones, it is recommended that you eat low-fat, high-fibre foods such as fruit, vegetables, whole grains, low-fat dairy products and legumes, and avoid fatty, fried and heavily processed stuff. It is also important to ensure adequate fluid intake: drink at least 2 liters of fluid per day to increase the flow of bile and help to remove the concrements.
The disease can be provoked by too much digestible carbohydrates. Sugar, fructose (which is found in soft drinks, juices and sweetened commercial foods) and white flour products should be used in moderation.
Bread and pasta made from whole-wheat flour and foods rich in natural carbohydrates, such as whole-wheat whole-grain rice or jacket potatoes, should be given preference.
Conclusions
The main thing you should know about gallstone disease is that the presence of crystalline masses in the gallbladder is not a problem in itself, but it will become one as soon as the body starts to give alarm signals, such as a feeling of severe discomfort after meals and abdominal pain, especially attack-like and long-lasting. In this case, the disease requires urgent medical care, because an even more severe attack can occur unexpectedly and at the most inopportune moment, leading to serious consequences. Stones in the gallbladder, as a rule, are not possible to dissolve; and organ-sparing ways to «get them out» of there simply do not exist. A timely and efficiently performed cholecystectomy surgery will get rid of the disease once and for all. Whenever there are doubts, or additional arguments are needed to make a decision, you can seek a second opinion from world-class specialists.
References
- S3 -Leitlinie Diagnostik und Therapie von Gallensteinen der Deutschen Gesellschaft für Verdauungs- und Stoffwechselerkrankungen und der Deutschen Gesellschaft für Viszeralchirurgie. In: AWMF online
- Treatment for Gallstones. National Institute of Diabetes and Digestive and Kidney Diseases. November 2017.
- "Symptoms & Causes of Gallstones | NIDDK". National Institute of Diabetes and Digestive and Kidney Diseases. Retrieved 2022-06-28.
Comments — 1
Людмила
Отличная и поучительная статья.