
Hallux valgus, commonly referred to as "bumps" or "bunions" on the feet, is a common orthopaedic problem. It causes pain and makes you give up elegant shoes. Let's understand the causes, as well as various treatment options for a very common, yet a very troublesome condition.
How do I know if I really have hallux valgus?
The Latin term “hallux abducto valus” was first used for this condition by the German surgeon Karl Hüter in 1870. It is translated as "outwardly withdrawn thumb". Currently, a shorter version consisting of only two words is used. Either way, it is a deformity of the first (big) toe, in which the first metatarsal bone diverges from the second and bulges out.
In severe deformities, the big toe itself also becomes crooked. In these cases, the nail turns inwards. Another noticeable change is the deviation of the big toe towards the neighbouring toes, which makes the foot curve.
Typical complaints and possible complications
The most common pain is caused by the bunion rubbing against the shoe. Bruising occurs, sometimes accompanied by inflammation of the synovial bag in the joint area (bursitis).
Due to the incorrect position, the support function of the foot is impaired. Painful calluses are formed and the weight gets shifted to other toes that are much less suited to bear it. Even so-called fatigue (stress) fractures sometimes occur.
The outward pointing big toe forces the small toes to bend, which eventually leads to claw toe and hammertoe deformities of the others. The second toe is forced upwards, and the constant pressure can end up tearing the ligaments of the metatarsophalangeal joint (plantar plate). As a result, dislocation occurs, and the second toe is shifted inwards? Extending over the next (the so-called overlapping toe). All these changes cause severe pain to the patient.
What causes finger deviation, and can it be prevented?
There are several theories as to what may cause the abnormal condition, one of which is hypermobility of the big toe.
This feature is characteristic of primates and is the reason why monkeys can grasp objects with their lower limbs. More precisely, it happens due to the fact that its tarsal joint allows for rotational movements. The human foot has lost this ability in the course of evolution: in humans this joint is immobile and serves only to redistribute the load.

In those with valgus deformity, this function is to some extent preserved. Therefore, the predisposition to develop the condition is congenital. It may manifest itself already in childhood and is inheritable. For some reason, women are much more often affected than men.
There are no effective ways to prevent unwanted changes. Bandages, orthoses or toe extensors can bring temporary relief, but do not exclude the possibility of "bumps" or stop the progression of the disease.
What are the best shoes to wear for valgus deformity of the big toe?
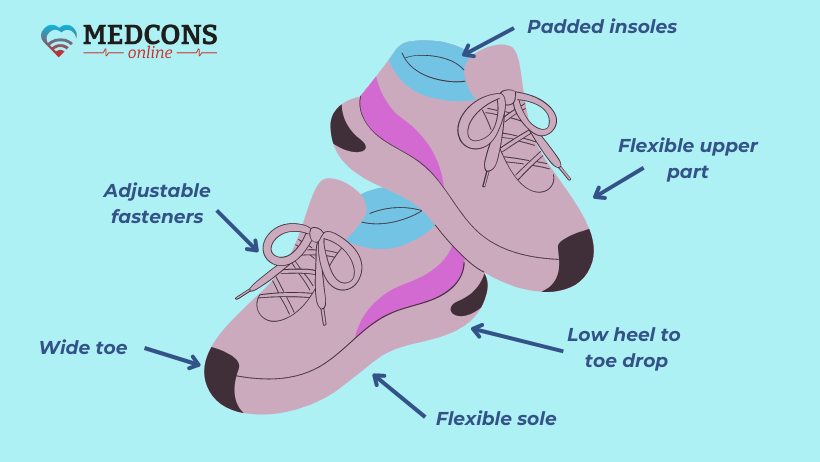
The best shoe suitable for such a condition is the one that reduces pressure on the forefoot, supports its natural mechanics and provides adequate space for the toes. Here are some characteristics that are important when choosing the right shoe for people with hallux valgus:
- A wide toe provides adequate toe space, which helps reduce pressure and allows for a more natural toe position.
- A low instep (difference between heel and toe height) minimizes pressure.
- A flexible sole provides natural movement and helps strengthen the foot muscles.
- Cushioned insoles absorb shock and increase comfort, especially if pain is present.
- Adjustable closures (velcro or laces) provide custom fit and better support.
- Soft and elastic upper materials prevent pressure points and increases comfort.
- Customized orthopaedic insoles support muscles and stabilize gait.
What examinations are necessary to diagnose the disease?
A clinical examination is sufficient to make a diagnosis. With the help of it, an experienced physician shall determine the degree of deformity and mobility of the first metatarsophalangeal joint, detect signs of osteoarthritis, excessive mobility of the first toe and misalignment of the little toe. This diagnostic method also provides important information for possible surgery, including assessment of blood circulation, sensory disorders (polyneuropathy), hindfoot abnormalities (e.g. fallen arch, shortening of the Achilles tendon, etc.).
Radiological examination of the foot under load (standing position) provides additional essential data for the choice of surgical treatment.
Hallux valgus and hallux rigidus: what is the difference?
Rigid big toe (hallux rigidus) "competes" with valgus deformity, ranking only slightly below in frequency. Both disorders affect the big toe and have similar manifestations. However, while in the case of hallux valgus it is only an incorrect toe form, hallux rigidus is thinning of the articular cartilage (arthrosis). Notably, the former condition can cause the latter.
Stages of valgus curvature
Depending on the nature of the changes, three stages of the disease are distinguished.
| Stage | Toe position | Bunion position |
| I | starting to shift inwards | not protruding |
| II | distinctly inward | protruding |
| III | displaced to an extent that it overlaps the neighbour | Severely protruding outwards |
Are there any conservative treatments available?
In the early stages, symptoms can be relieved without surgery. Wearing shoes that provide enough space for the foot reduces friction. Silicone spacers can also be used to protect the curved toes from friction, but they do not correct the deformity.
Custom insoles can provide some relief. Various physiotherapeutic methods, above all the disease-specific exercise programs, also show good results.
When is surgery necessary?
In most cases, surgery is recommended if the pain cannot be relieved by conservative measures, constant friction leads to the formation of painful pressure points and calluses, as well as malposition of the other toes.
The exception is when it is too pronounced, and can lead to arthritis unless corrected.
As for children, most experts believe that due to the high recurrence probability, surgical treatment should not be used until the end of the child's growth period.
What kind of surgeries are there?
Surgical treatment is the only way to correct the deformity and get rid of the pain. To date, more than 100 methods have been described. Choosing the best option that will provide the best result in each specific situation is a task that can only be achieved by very experienced orthopedics experts specializing in foot issues.
The aim is to correct all existing defects (e.g. concomitant curvature of the little toe and/or hindfoot) in a single operation.
In all cases, the procedure involves the bones and is essentially an osteotomy, which is separation of bones. It is not possible to straighten the big toe by working on the soft tissue alone.
The operation can be performed in a standard, open-surgical technique, or minimally invasive. The second option is preferable, but is only offered by facilities and doctors with the appropriate level of expertise.
Minimally invasive chevron (V-shaped) osteotomy combined with Akin osteotomy
Indications: mild to moderate deformity. The surgery is usually performed under general anaesthesia, but spinal or local anaesthesia is also possible.
During the procedure, the patient lies on his back and the sterile washed and covered foot is placed on an X-ray machine, which is used to monitor all further actions. This eliminates the need for exsanguination of the operative field, so the thermal effect on the bone is minimal and postoperative oedema is reduced.
The first stage is a chevron osteotomy.
A 2 cm long incision is made on the inside, just in front of the protruding ossicle. A minimally invasive dilator with a thin tip is inserted into the bone through the incision. During its operation, the skin is cooled with a water jet to prevent thermal damage.
Next, a V-shaped dissection of the head of the first metatarsal bone at its neck is performed. The joint is not opened, which prevents its postoperative stiffness.
A special instrument is then inserted into the bone body through a small incision to move the head outwards.
For fixation, cannulated screws are used to ensure precise positioning of the fixation material. One of them is fixed obliquely in two places on the metatarsal bone and the other is inserted into the head of the bone through the medullary canal. The protrusion resulting from the displacement of almost one bone width is removed with a bone cutter.
The next step is the Akin osteotomy. Through a small incision at the base of the thumb, the proximal phalanx is separated and the thumb is straightened. This position is fixed with a special bandage (taping).
Six weeks after the operation, an X-ray examination is done to make sure that the bone is completely healed. The tapes can then be removed and normal shoes can be worn. From this point on, patients are advised to perform daily toe movement exercises. The aim is to achieve a 90° extension of the metatarsophalangeal joint.
Lapidus arthrodesis
Indications: severe deformity and instability of the tarsal joint.
This surgical technique has the greatest potential for correction in cases where the gentler option described above is no longer possible. However, arthrodesis is contraindicated in advanced stages with severe wear and tear of the metatarsophalangeal joint.
During the operation, the patient lies on his back on the operating table under general anaesthesia. The first step is to dissect the capsule of the metatarsophalangeal joint from the outside. This is done through a small incision in the space between the toes. An incision about 10 cm long is made above the 1st toe bone.
The joint is exposed, its surfaces are carefully scraped and the wedge protruding part of the bone is removed. The first metatarsal bone is connected to the tarsal bone and thereby pulled outwards. The position is temporarily fixed with two wires.
An angular stability plate is then attached to the sole side, after which screws are inserted. One of them crosses the connection point. The other screws have a threaded head, which is screwed into the plate to ensure additional stability.
The surgeon opens the metatarsophalangeal joint of the big toe through an L-shaped incision in the capsule, removes the convex part of the head, reduces the volume of the inner part of the capsule and closes the wound.
After the operation, a bandage shoe must be worn for six weeks to immobilize the foot, and the foot can bear the full weight from the first postoperative day. It is recommended to wear a shoe with an instep on the other foot to make the length of the limbs equal.
After six weeks, X-rays are taken to confirm complete bone healing, after which normal shoes can be worn.
Patients are encouraged to keep the leg in an elevated position, avoid long walks; lymphatic drainage is also helpful.
Open chevron osteotomy
Indications: Mild to moderate valgus deformity. The head of the first metatarsal bone is dissected through a 5 cm long "V" shaped incision, shifted outwards and fixed with a screw. The intervention involves not only the bones but also the soft tissues: the joint capsule and tendon on the outside of the big toe are dissected and the inner part of the capsule is sutured.
Relative contraindications are instability of the metatarsophalangeal joint or a very narrow metatarsal bone.
An unpleasant consequence, as with any other open surgery, is some limitation of movement in the metatarsophalangeal joint of the big toe. Another disadvantage of the method is that the correction potential is not very high.
Reverdin-Green procedure
This technique is indicated for mild to moderate hallux valgus with curvature of the articular surface. The metatarsal bone is cut close to the toe, as with an open chevron osteotomy. A wedge-shaped hole is sawed out on one side. The head is pushed outwards and rotated so that the articular surface is aligned perpendicular to the longitudinal axis of the metatarsal bone.
Z-shaped ("scarf") osteotomy
The word "scarf" in the name of the operation describes the shape of the bone incision made by the surgeon. The tarsal bone is cut in a "Z" shape, the head is shifted to the outside and fixed with two screws. This method makes it possible to correct a more severe deformity, but it is much more complicated than the previous ones.
Osteotomy of the first metatarsal base
In case of a pronounced dislocation with a severe deviation of the 1st ray, the metatarsal bone is dissected near the base in the form of a wedge. After removing the wedge, the metatarsal bone is turned outwards and fixed with a plate and screws.
Another option is a straight dissection of the bone when a triangular gap is created by turning the metatarsal bone outwards. Fixation is done with a plate with a pin in the gap area.
Theoretically, these methods can correct a high degree valgus deformity without damaging the metatarsophalangeal joint. However, the disadvantages are a high rate of recurrence and impaired healing, as well as pain in the area above the plate, which results in its removal.
The Bösch technique
A special feature of this method is innovative fixation. As with the minimally invasive chevron osteotomy with Akin osteotomy, the metatarsal bone is dissected through a small incision on the outside of the joint and pushed outwards. A wire is inserted into the outside of the big toe, which is advanced along the bone into a recess and then brought through the skin to the outside. After about 6 weeks it is removed in a painless procedure that does not require anaesthesia.
However, the end of the wire is left exposed, which can be uncomfortable and has a theoretical risk of infection.
The Stofella procedure
In this case, a fixation method is also used. The osteotomy is performed through a small incision on the outside of the joint. After shifting, the correct position is fixed with an intramedullary implant. This consists of a component that extends into the bone and a component that is screwed onto the head.
The advantages here are also the extra-articular osteotomy, reduced post-operative joint stiffness and only one small incision. However, after correction, a bony protrusion remains at the level of the osteotomy site, only a small part of which can be removed without compromising stability. Another disadvantage is the relatively large implant and the location of the screw-retained component on the inside of the head. For this reason, the implant often has to be removed in a second operation.
How successful can hallux valgus correction be?
If the most appropriate technique is used and everything is done correctly, complete correction can be achieved permanently in more than 95% of cases. The likelihood of recurrence in most cases depends on the surgeon’s skill, correct choice of surgery method and technical implementation. This is why the success rate is very high at specialized facilities, while at non-specialized ones, on the contrary, it can be no more than 30-50%.
Which doctor should I see for protruding bunions on my feet?
In principle, foot issues are taken care of by both orthopedists and podiatrists. A podiatrist is not a doctor, but deals with, for example, ingrown toenails or the removal of corns; they can recommend insoles, provide physiotherapy and advice on foot care, and see which cases require surgical intervention. When it comes to treatment, the help of an orthopedist is needed, ideally of a foot surgery specialist.
Correction of valgus deformity requires a very good knowledge of the anatomy, physiology and physiopathology of this part of the musculoskeletal system. Practical experience is also important.
Only in this case you can be sure of a sufficient level of expertise. It is officially confirmed by certificates granted by professional associations.
Often such surgeons are also sought for a second opinion on foot conditions, which, if facilitated by a specialized service, can be provided remotely. Such advice helps to get a more accurate idea of the possible ways to correct the defect, to choose the best surgery method, or to plan an in-person surgery appointment.
References
- Jörg Halfmann. Der Hallux valgus. Reihe "Den Fuß verstehen". Podo-Taping-Academie, ISBN 978-3-00-060961-9, 1. Auflage 2019
- Tonio Gottlieb. Hallux valgus Deformität. In: Der Fußchirurg. Dr. med. T. Gottlieb, 24. Juni 2021
- Vincent J. Hetherington. Hallux Valgus and Forefoot Surgery. Churchill Livingstone, 1994 ISBN 044308775X, 9780443087752
Comments — 0