

In most cases, malignant kidney tumors arise from the epithelial cells of nephrons (the basic elements of the renal structure) and represent renal cell carcinomas. As a rule, the disease affects only one part of the paired organ and is often detected by chance.
Causes
The causes of kidney cancer are still not precisely understood. However, certain factors are known to increase the risk of developing it.
Smoking
It is known that nicotine can provoke the disease. The likehood of getting it increases with the number of cigarettes smoked per day and the duration of smoking. Not only active smokers but also passive ones are affected.
Medication
It is believed that regular use of certain painkillers, especially those containing phenacetin, which causes kidney damage, can also cause renal cell carcinoma.
Genetics
Approximately one in 100 patients has a genetic predisposition to developing this type of cancer. It can be inherited. The onset of the disease at a fairly young age (before 30-40 years of age) is a good reason to assume that it is hereditary.
Such genetic changes are characteristic of Hippel-Lindau disease, a rare hereditary syndrome in which benign and malignant neoplasms affect a variety of organs. Between 28 and 45 per cent of patients with this pathology also suffer from kidney cancer.
Patients with tuberous sclerosis (tumor-like changes in various organs caused by pathogenic mutations) are also at risk.
Chronic diseases and lifestyle
Unfavourable factors include overweight, high blood pressure, chronic inflammation of the urinary system and chronic kidney failure requiring dialysis. Occupational exposure to toxic substances/carcinogens (trichloroethylene, cadmium and its compounds, aryl or alkyl halide) can also lead to kidney cancer.
Classification
Malignant tumors found in the kidneys may be primary or secondary (i.e. metastases from a primary site located in another organ). A distinction is also made between unilateral and bilateral cancers, the latter one being either asynchronous or synchronous (if no more than 6 months have elapsed between the detection of the first and second mass).
Origin
Most often malignization occurs in the cells of the functional renal tissue (parenchyma), more specifically in its smallest structural units (nephrons). Accordingly, this type is called renal cell cancer (carcinoma or adenocarcinoma).
There may also be malignant masses in the kidney that did not arise from the renal tissue. For example, lymphomas (lymphatic cancer) and sarcomas that develop in muscles. These rarely occur in adults, as do nephroblastoma (Wilms tumor), which almost exclusively affects only children under the age of five.
Renal cell cancer, in turn, is divided into subtypes depending on the original tissue, cytogenetic findings and histological features. A distinction is made between clear-cell, chromophilic (papillary) or chromophobic carcinomas, and Bellini duct carcinoma.
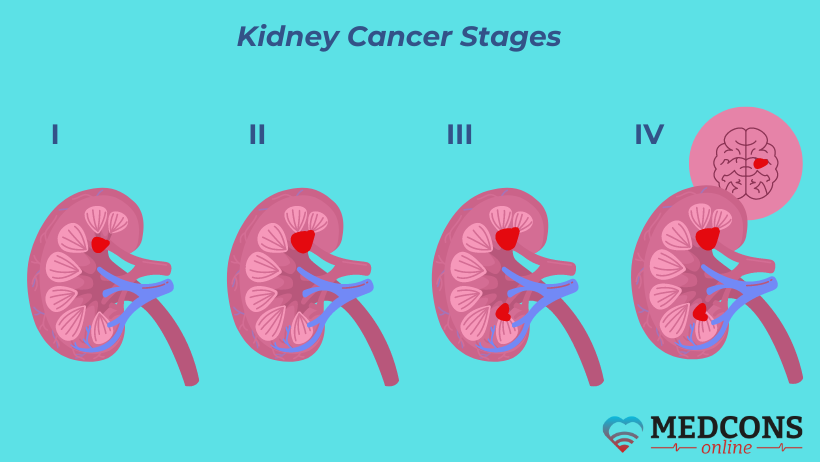
Extent of cancer (stage)
The following international TNM-classification values are used for kidney cancer staging:
| T | Tumor size and spread |
| Т1 | Up to 7 cm and within the organ |
| Т2 | Over 7 cm and within the organ |
| Т3 | Infiltrated into large veins, adrenal glands or nearby adipose tissue without crossing Gerota's fascia* |
| Т3а | Infiltrated into the adrenal gland or nearby adipose tissue |
| Т3b | Infiltrated into the renal vein(s) or inferior vena cava below the diaphragm level |
| Т3c | Infiltration into the vena cava above the diaphragm |
| Т4 | The tumor extends beyond Gerota's fascia |
* the fibrous layer surrounding the kidney and the adipose capsule
| N | Lymph Nodes | M | Metastases |
| N0 | Without lymphatic spread | M0 | No distant metastases |
| N1 | Metastases in one regional lymph node | M1 | Evidence of distant metastasis |
| N1 | Metastases in several lymph nodes |
The size of the tumor and its progression inside and outside the organ are of fundamental importance.
Based on the TNM characteristics, the stage of the kidney cancer is determined:
|
First: T1N0M0 |
|
Second: T2N0M0 |
|
Third: T3N0 or T1-3N1M0 |
| Fourth: Any tumor which has grown through Gerota's fascia /metastases to more than one lymph node / distant metastases |
Symptoms of kidney cancer
The disease is asymptomatic in its early stages. Therefore, very often (in about 70% of cases) it is detected accidentally, for example, during an ultrasound examination carried out for other reasons. Complaints occur only at later stages, and not all of them are specific (that is, characteristic of a certain pathology).
In rare cases, malignant masses may be palpable.
The presence of a malignant condition may also be indicated by other manifestations such as:
- unintentional weight loss;
- loss of appetite;
- fatigue;
- anaemia;
- persistent or frequent fever;
- first observed increase in blood pressure;
- swollen legs.
In men, a kidney tumor can provoke a rupture of a varicose vein in the testicles.
Complications
The main consequence of advanced malignant kidney disease is damage to other organs and structures. Metastases may spread to lymph nodes, the adrenal gland or the inferior vena cava wall, as well as further to the lungs, bones, and, less frequently, the brain and liver.
Diagnosis
Before proceeding with more complex tests, the doctor will ask the patient about complaints and symptoms. If kidney carcinoma is suspected, special attention is paid to its typical manifestations, such as blood in the urine. Physical examination also includes palpation of the lumbar region. Laboratory and imaging tests are then performed.
Urinalysis
Since in the early stages of the disease the amount of blood in the urine is usually so small that it is not visible to the naked eye, the urine should be tested for blood admixture using test strips. These accurately detect even the smallest amount of blood, or more precisely, small amounts of the blood pigment hemoglobin in red blood cells.
Blood tests
Malignant renal processes can cause specific changes in the blood. For example, all cancerous conditions may cause a decrease in the number of red blood cells. In contrast, kidney cancer often increases the levels of the hormone erythropoietin, which stimulates the formation of red blood cells. Therefore, the number of red blood cells increases. However, to date, there is no known blood substance produced by cancerous or healthy renal cells in response to a tumor, and that can be used as its indicator (tumor marker). Therefore, blood tests (in particular, complete blood count, creatinine, urea, calcium, alkaline phosphatase, LDH, liver function panel) are used to obtain additional information about the function of important organs and systems rather than for diagnosis.
Ultrasound
Abdominal sonography is performed to assess the shape and structure of the kidneys. This allows the detection of external changes in the organ, indicative of a tumor, at an early stage. At later stages, ultrasound helps to determine how far the mass has spread.
Computed tomography
A CT scan can provide a more accurate image of the affected kidney and the possible spread of the tumor. It can clarify ambiguous ultrasound findings and detect metastases to nearby organs such as the liver, pancreas and neighboring lymph nodes. A computed tomography scan with contrast is currently the gold standard for the diagnosis of kidney masses.
Magnetic resonance tomography
In case of allergy to contrast agent or renal insufficiency, magnetic resonance imaging is an alternative to CT. It may additionally be performed to visualize parts of the tumor protruding into the renal vein or vena cava, which may be necessary in surgery planning.
Chest X-ray and CT scan
A chest x-ray (X-ray or CT scan) is used to look for possible lung metastases.
Biopsy
Tissue sampling is not a standard procedure in renal tumor diagnosis, but should be performed to determine its specific features in the following cases:
- if CT/MRI findings are inconclusive;
- if the watch-and-wait approach is considered as an option for a very small mass;
- if local therapy using radiofrequency ablation or cryotherapy is possible.
Sampling uses a hollow needle that is inserted through the skin into the tumor tissue under local anaesthesia and under ultrasound or CT guidance.
Other diagnostic procedures
Bone metastases can be detected by a bone scan. In some cases, it becomes necessary to assess the blood supply to the kidney before surgical removal of a kidney mass, which is done with the help of angiography. If secondary lesions in the brain are suspected, an MRI or CT scan of the brain is needed. In the case of poor renal function, only one functioning kidney, or if there are potentially dangerous co-morbidities such as diabetes or high blood pressure, further tests may be required to evaluate the kidney function.
Kidney cancer treatment
A thorough examination and disease staging help the doctor to assess the situation as accurately as possible and to determine the best therapeutic strategy. The choice depends, in particular, on the extent of tumor spread at the time of diagnosis. The age and general health of the patient are also key factors.
Surgical resection
Among the many possible treatment options, surgery is of major importance. The aim of an operation is to completely remove the tumor and thereby cure the disease. However, surgery for this purpose is usually only possible if the tumor has not spread outside the organ. If it has already invaded the surrounding tissues and lymph nodes or even spread to other organs, surgery is usually only appropriate in combination with other therapies.
Organ preservation surgery
It is now well known that organ preservation tumor removal has clear advantages even in patients whose other kidney is healthy. There is convincing evidence that patients operated on in this way are less likely to die, for example, from cardiovascular disease. The risk of recurrence is no higher than after radical resection.
The feasibility of this technique depends on the tumor location, growth and size.
In this case, it can usually be separated from healthy renal tissue, leaving the rest of the kidney intact, so that it retains all its functions.
Organ-sparing surgery is absolutely necessary if the patient has only one kidney left or if the other kidney is not working properly.
If the tumor can be completely removed and kidney function is not impaired, no further treatment is required.
Removal of the entire kidney affected by cancer (nephrectomy)
In the case of larger or unfavorably located lesions, the entire organ together with the surrounding adipose capsule must be removed (radical nephrectomy). Radical nephrectomy is also performed when the cancer has infiltrated the renal pelvis or when blood clots (thrombi) have formed in the renal or inferior vena cava veins, as well as in the presence of metastases (i.e. at stages 3 and 4), unless there are contraindications related to general health and vital organs.
Radical surgery also involves resection of the nearby lymph nodes.
When nephrectomy is performed at an early stage (without lymphatic and distant metastasis), the chances of recovery after surgery are relatively high. At stages 2 and 3, the procedure still has a curative purpose. In cases of metastasis, the affected kidney is removed to reduce the total tumor burden in the body (so-called cytoreductive surgery) or as a palliative measure (to relieve symptoms). In such cases, surgery is followed by systemic therapy to control the tumor spread.
Surgical techniques
Generally, both organ preservation operations and total nephrectomy can be done by open surgery (through a standard abdominal wall incision) or laparoscopy (through small incisions). The minimally invasive procedure has more benefits in terms of the healing process, and robot-assisted technology is considered the preferred option to perform it.
The choice depends on the individual characteristics of the tumor and the patient’s anatomy.
Local treatment (thermo- and radiofrequency ablation, cryotherapy)
For small tumors located on the outside of the organ, local therapy may be an option. In this case, the mass is punctured from the outside and exposed to cold, heat or high-frequency alternating current. Such procedures are particularly suitable for patients who wish to avoid surgery or cannot tolerate surgery due to severe comorbidities. The disadvantage of the method is that it is not possible to perform a pathological examination of the exposed tissue to make sure that the affected area is completely removed.
Renal artery closure (embolization)
Arterial embolization may be offered to patients in severe general condition who are contraindicated for surgical treatment. The procedure involves blocking the blood vessels that supply the tumor. The aim is to slower its growth and relieve the symptoms of the disease.
Watch and wait
Various studies have shown that masses smaller than 2 cm are often relatively low-grade, i.e. not very aggressive, and grow slowly. Therefore, initially they can simply be closely monitored with CT or MRI. If imaging reveals changes, one should change monitoring for active action.
Drug therapy for renal cell cancer
If the cancer has progressed after initial treatment, or if metastases are already present at the time of diagnosis, systemic drug therapy is necessary.
The most common and well-studied classes of targeted drugs are tyrosine kinase inhibitors and mTOR inhibitors. They act by blocking growth factor receptors, inhibiting the formation of new tumor cells. With the exception of the mTOR inhibitor temsirolimus, all drugs are taken orally as tablets, which means there is no need to stay at hospital for treatment. Temsirolimus is administered intravenously as an outpatient.
Targeted therapy also includes treatment with antibodies to VEGF (bevacizumab + interferon). Due to the relatively complex administration (intravenous and subcutaneous self-injections) and side effect profile, this therapy is rarely used.
The newest drug for the treatment of metastatic renal cell carcinoma is the PD-1 inhibitor nivolumab. It is an antibody that blocks the so-called programmed death-1 (PD-1) receptor. It binds to the PD-1 receptor on T-cells and suppresses interaction with PD-L1 and PD-L2 ligands on tumor cells. Thus, it stimulates the immune system and acts as an indirect antitumor agent.
There is still no definite opinion on the optimal sequence of medications and on which one is the best for a particular patient in a particular situation. Ultimately, the decision depends on many different factors - general condition, treatment already performed, risk group, individual drug tolerance and the treating physician’s experience.
Prognosis and prevention
The 5-year relative survival rate for renal cell carcinoma is 77% in men and 79% in women. Thus, the prognosis is considered quite favorable. Patients with very small tumors have an even better chance of cure, i.e. more than 90%. The good news is that almost half of all malignancies are diagnosed at a relatively early (first or second) stage.
In general, the course of the disease depends on a number of factors - age, physical status, size and spread of the tumor at the time of diagnosis. As with all other cancers, the rule is, the earlier the evil is detected, the easier it is to fight it. Therefore, regular screening examinations are of great importance for the prevention of kidney cancer. Almost all body check programs include ultrasound examination of the abdominal cavity.
And the risk group patients are strongly encouraged to undergo regular ultrasound examinations starting from the age of 45.
Correcting your lifestyle, that is, giving up smoking, weight and blood pressure control can also help prevent malignant renal processes.
Second Opinion
In contrast to other cancers, renal cell carcinoma is usually diagnosed by imaging rather than by histologic examination. It is well known that imaging data can be interpreted in different ways. Therefore, at the stage of making this diagnosis, it is important to be confident in the correct evaluation of ultrasound or CT findings. The expert opinion of an experienced radiologist or urologist can help.
The critical importance of imaging is also linked to another problem that patients often cannot resolve with their treating physicians. This concerns allergies to contrast or the danger of administering contrast agent due to poor kidney function. The way out of such seemingly dead-end situations can be suggested by specialists with more solid clinical experience.
A second opinion on renal cancer is indeed also necessary when planning surgery. Without special knowledge, it is difficult to understand the variety of methods and options for surgery on your own. Is it better to try to remove only the tumor, or would removing it together with the entire kidney be a more reliable option? Is it worth striving for an opportunity to operate with the help of a robot-assisted system, or can one rely on time-tested standard surgical technologies? Consulting a reputable specialist, which can be not only in-person, but remote, will help you make an informed decision and give you confidence that it is correct.
References
- Munoz, J.J., et al. Upper tract urothelial neoplasms: incidence and survival during the last 2 decades. J Urol, 2020. 164: 1523.
- Rationelle Diagnostik und Therapie in der Inneren Medizin in 2 Ordnern; Hrsg.: J. Meyer et al.; Elsevier, 11/2018
- Oberneder R et al: Nierenzellkarzinom. Manual Urogenitale Tumoren. Tumorzentrum München und Zuckschwerdt-Verlag München. 4. Auflage 2008
- Integrating On-Treatment Modified Glasgow Prognostic Score (mGPS) and Imaging to Predict Response and Outcomes in Metastatic Renal Cell Carcinoma; JAMA Oncology; Published online June 22, 2023; doi:10.1001/jamaoncol.2023.1822
- Schrenk F et al: Nierenzellkarzinom. Aus: Das Rote Buch. Berger DP et al (Hrsg). 4. Auflage 2010 Ecomed
Comments — 3
Наталья
Я, как пациентка, и медработник, прочитала новую информацию. С каждым разом, уверенность в излечении увеличивается.
Валерий Алёхин
Доброго дня! Три года назад мне полностью удалили правую почку, был рак, без метастазов. Регулярно прохожу контрольную диагностику, но не оставляют мысли о том, что рак может поразить и вторую почку. Есть ли какие-нибудь надежные методы контроля и профилактики, чтобы уверенно можно было исключить повторение полезни?
Наталия Соловьева
У моего брата после операции рака почки недержание мочи и кала. Говорят, такое случается редко, но брату от этого не легче. Спасибо Medconsonline за совет Вашего врача делать гимнастику на мышцы таза, прямо на глазах лучше становится.