

The disease, like many other dangerous conditions, is almost undetectable in its first stages. It is generally believed that liver cirrhosis is related to alcohol, but there may be many more causes. It is extremely important to undergo treatment, otherwise the disorder can be fatal due to progressive liver damage.
Description of the disease
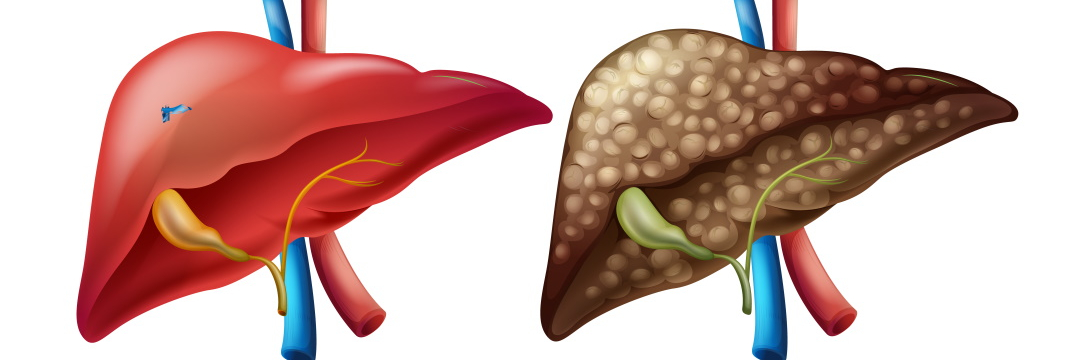
In the initial stages, there is an overgrowth of liver connective tissue (fibrosis) with the formation of nodules from 3 mm to 3 cm. Due to this transformation, the organ ceases to adequately fulfil its tasks, such as metabolic and detoxification functions. Chronic liver failure occurs. Cirrhosis is the final stage of the disorder.
What are the liver cirrhosis symptoms?
In most cases, the disease is first asymptomatic. Destructive changes, ending in cirrhosis, occur almost imperceptibly. Sometimes abnormal findings in blood tests or ultrasound are detected accidentally, during a routine examination.
What happens later?
Fatigue, nausea and loss of appetite are the late-stage liver cirrhosis symptoms. Skin changes add to these non-specific signs, including:
- spider-like blood vessels, especially on the face or upper body;
- itching;
- white spots on the nails;
- redness and thickening of the palm tendons;
- blood vessel dilatation;
- redness and paling of the lips and tongue.
In men, they can be manifested by loss of hair on the abdomen and impotence, a decrease in the size of the testicles and enlarged mammary glands; in women – by irregular menstruation.
Disease progression and complications
Additional symptoms may appear with time, such as:
- yellowing of the skin and eyeballs, dark urine, pale stools (jaundice);
- fluid retention in the abdomen and legs;
- shortness of breath;
- nosebleeds;
- severe weight loss;
- deterioration of brain function.
There is also increased pressure in the portal vein, which carries venous blood from the abdomen to the liver. The smaller veins become congested and dilated. This leads to stomach and oesophagus bleedings. There is an increased risk of liver cancer as a late consequence of chronic liver damage.
Another complication is the accumulation of fluid in the abdominal cavity. This causes abdominal pain and difficulty breathing.
If the affected organ ceases to sufficiently cleanse the blood of toxins, they reach the brain, causing mental and neural disorders and hepatic encephalopathy.
Causes
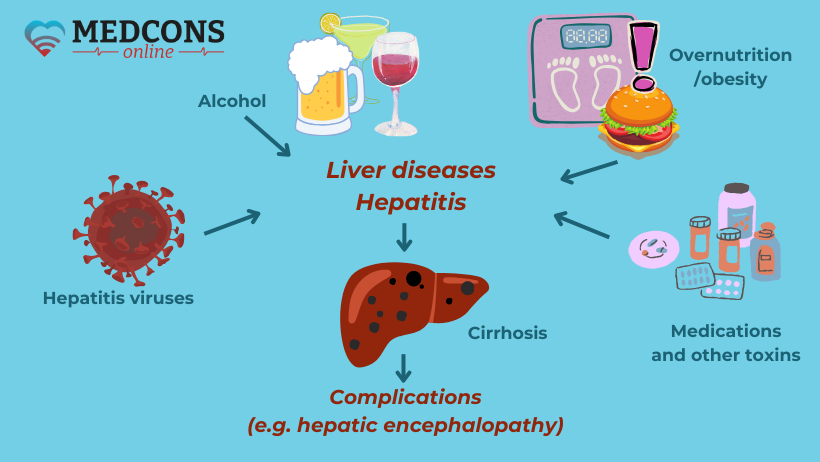
Nonalcoholic fatty liver disease (steatosis) is one of the most common liver diseases. It occurs when the body gets more energy than it needs. The excess is stored as fat, including in the liver. Usually, fatty hepatosis is the result of a metabolic syndrome characterized by obesity, poor metabolism of fats and sugar, hypertension. It can develop into chronic inflammation and subsequently into cirrhosis.
Long-term alcohol consumption at a certain stage can also lead to the development of steatosis, which in this case is called alcoholic fatty disease.
A significant part of liver cirrhosis cases is caused by type B and C viral hepatitis. Less frequently, other infectious diseases, as well as cystic fibrosis, autoimmune inflammation, and medication side effects can lead to the development of the disease.
Diagnosis
Early detection of the disease is of crucial importance, as it allows for timely treatment and prevention.
The simplest method is palpation. Enlarged liver and spleen may indicate a dangerous process.
Laboratory tests
|
Albumin, coagulation factors, cholinesterase. |
↓ |
|
Bilirubin |
↑ |
|
Platelets, white blood cells. |
↓ |
|
Transaminases |
↑ |
| Ammonia | ↑ |
Imaging tests
Abdominal ultrasound reveals cirrhotic changes on the liver surface, as well as specific complications (abdominal hydrocele, enlarged spleen, new vessel growth).
Doppler sonography can determine the degree of portal hypertension.
Other modern non-invasive diagnostic techniques are used to measure liver stiffness at different stages (fibroscan/transient elastography and shear wave elastography), as well as fat content in liver cells (steatoscan).
In complicated cases or if the ultrasound results are contradictory, a CT or MRI is performed. They are not much more effective than ultrasound, but more accurately identify cancer-like foci in the cirrhotic liver.
Differential diagnosis
Since changes in the structure of the liver can also be a sign of cancer, it is sometimes necessary to take a tissue sample (biopsy) for diagnosis. For this purpose, an ultrasound-guided puncture or minimally invasive surgery (minilaparoscopy) is performed.
Stages of the disease
Staging is done according to the Child-Pugh-Score, which analyzes the disease according to five criteria and scores it according to a point system.
|
Category |
Number of points |
Liver function |
|
Child-Pugh-A |
5 |
good |
|
Child-Pugh-B |
7-9 |
medium |
| Child-Pugh-B | 10-15 | bad |
By summing up the scores, the doctor assigns the disease to a certain class. It determines therapy planning and prognosis assessment. At the Child-Pugh A stage, the prognosis is still quite favorable; as the disease progresses and the total score increases, the prognosis worsens.
Treatment of liver cirrhosis
Unfortunately, the scarring characteristic of liver cirrhosis is irreversible. However, it is often possible to stop the progression of the disease and combat symptoms and complications with therapeutic measures.
The type of treatment depends on the cause of the disease. For example, the best option for alcoholic cirrhosis is abstinence from alcoholic drinks. In the case of hepatitis C and B, drug antiviral therapy is necessary, and in the case of autoimmune hepatitis, drugs that suppress the immune system are used.
Management of complications
Of course, therapy should not only stop the progression of the disease, but also treat its complications.
Ascites and edema. In ascites and edema, the first thing to do is to limit fluid intake. A low-salt diet is also necessary, since the sodium contained in table salt contributes to water retention. Diuretics are prescribed to accelerate fluid discharge.
When medications do not help sufficiently reduce the volume of fluid in the abdominal cavity, it is removed by puncture.
Spontaneous bacterial peritonitis. If examination of ascitic fluid reveals the presence of leukocytes or bacteria, antibiotics are administered.
Portal hypertension and varicose veins. Some beta-blockers developed to treat hypertension can lower blood pressure in the portal vein and in varicose veins in the esophagus and stomach. This reduces the risk of vein dilatation and rupture. If the chance of bleeding is too great, or if it has already occurred, the vessels are either ligated or sclerosed during a gastroscopy.
Liver encephalopathy. Protein-rich foods and bacterial breakdown products absorbed from the intestines worsen hepatic encephalopathy. In the past, a low-protein diet was prescribed. Now it is no longer recommended, since the intake of sufficient protein is necessary to maintain the patient’s general condition. However, the lactulose laxative can be very effective for patients with a tendency to encephalopathy, as it speeds up intestinal transit, preventing the absorption of too many bacterial breakdown products.
Liver cancer. The tumor is preferably removed by surgery. However, in the case of cirrhosis, it is usually impossible to remove the part of the organ with malignant foci, because the rest of the organ also has lesions that prevent is from fulfilling its function properly and recovering.
Another option is liver transplant. However, it may not be possible for a variety of reasons, for example, if there are metastases, the mass is too big, there are multiple malignant foci, or if the patient is in such a severe condition that he or she will not be able to tolerate such a big and complex procedure.
If a transplant is not being considered, or while waiting for a transplant, supportive therapy is usually given.
- Transarterial chemoembolization (TACE).
In this procedure, a catheter is inserted into the hepatic artery through which a chemotherapy drug, usually together with other substances that cause vessel occlusion, is delivered into the vessels supplying the tumor. The impact on the tumor is quite strong, while side effects on other organs are relatively minor. TACE is usually repeated every 6-8 weeks and may result in slower growth and sometimes a reduction in the size of the mass. Radiofrequency thermal ablation (RFA). In this procedure, a needle is inserted into the tumor from the outside and scleroses it by producing heat. The advantage of this method is that only one procedure is usually needed. Some patients can be cured with this treatment method.
- Radiofrequency ablation (RFA).
In this procedure, a needle is inserted into the tumor from the outside, and the cancer cells are killed by heat that it produces. The advantage of this method is that only one procedure is usually needed. Some patients can be cured with this treatment method.
- Percutaneous ethanol injection (PEI).
In this case, alcohol is injected into the tumor with a needle, resulting in the death of malignant cells.
- Systemic chemotherapy.
For liver cancer, no systemic chemotherapy has yet been found that could suppress tumor growth or prolong life. However, their search is ongoing, and substances are already known that could be used against hepatocellular carcinoma in the future. These drugs are already being offered in clinical trials to some patients for whom other treatments are not possible or have not had the desired effect.
Prognosis and prevention
The diagnosis as such does not mean the end of life. However, over time, scarring worsens, and the organ function continues to deteriorate. When the life-threatening stage is reached, a patient needs to find an alternative, and transplantation is the only remaining option.
To prevent the disease, the first thing to do is quit or at least moderate your alcohol consumption. The second most common cause of the dangerous illness can be eliminated with the help of vaccination against hepatitis. You should also be aware of occupational exposure to toxic chemicals, such as carbon tetrachloride, benzene, etc.
Cirrhosis patients are encouraged to take medications and vitamins only if they are really necessary. The liver, as the key metabolic organ, has to break down and eliminate all foreign substances from the body. Therefore, it is advisable to check with your doctor or pharmacist in advance how harmful a particular drug is for it. There may be a better tolerated substitute that does not increase the risk of liver damage.
Conclusions
Liver cirrhosis is a severe disease that develops gradually, the functional tissues being destroyed and replaced by connective onces. Eventually, scarring and reduction in size no longer allow the organ to fully perform its work.
The disease is usually irreversible. However, its progression can be slowed if the causes of the condition are eliminated. If there are complication signs, specific therapy is usually required. Very often, if it is not possible to eliminate the provoking factors, the only solution is liver transplantation.
References:
- Rationelle Diagnostik und Therapie in der Inneren Medizin in 2 Ordnern; Hrsg.: Meyer, J. & Pletz, M.W. & Mayet W.-J et al.; Elsevier, 5/2021
- Referenz Gastroenterologie; Hrsg.: Riemann JF, Fischbach W, Galle PR, Mössner J; Thieme-Verlag Stuttgart, 2019
- Essenzielles zur Leber; Hrsg.: Canbay A, Gerken G; MWV Verlagsgesellschaft Berlin, 2021
- Gastroenterologie für Intensivmediziner; Hrsg.: Canbay A, Gerken G; Thieme-Verlag Stuttgart, 2017
Comments — 0