


Prostate enlargement, or the so-called benign prostatic hyperplasia (BPH) is of the most common men’s health issues. It affects almost half of the male population over 50 years of age, and the incidence increases significantly with age.
In men younger than 40, the condition is rare, but in the age group from 50 to 60 years its frequency varies from 20 to 45% according to different data sources; after sixty its typical complaints become increasingly frequent, and after seventy they are present to some extent in 70% of men.
What is BPH and how does it manifest itself?
Frequent urges to urinate, the need to get up at night to go to the toilet and the feeling that the bladder is not emptied completely - these are the typical complaints with benign enlargement of the prostate.
Many men adapt to this condition and cope well with it. But for some it becomes a burden: they have to go to the toilet too often, to the point where they can't get enough sleep at night and become tired and sleepy during the day. In addition, having to urinate all the time can interfere with professional or other activities.
Most typical symptoms of prostate adenoma
If the prostate is distinctly enlarged, it puts pressure on the bladder and urethra. Therefore:
- the urge to urinate becomes more frequent and stronger than before, especially at night;
- it takes longer than before for the urine to come out;
- the stream becomes weaker and the act of urination lasts longer than before;
- urine continues to drip after urination and there is no sensation of emptying completely.
It refers to an increase in the organ’s volume accompanied by certain changes at the cellular level. The term "benign" emphasizes that it is not cancer.
There is not always a direct relationship between the size of the prostate and the severity of complaints. Some men with a very severe enlargement have only mild or very moderate complaints, while others may have major problems even with a slight enlargement.
Current evidence suggests that benign prostatic hyperplasia is not a precursor to carcinoma.
Causes BHP development
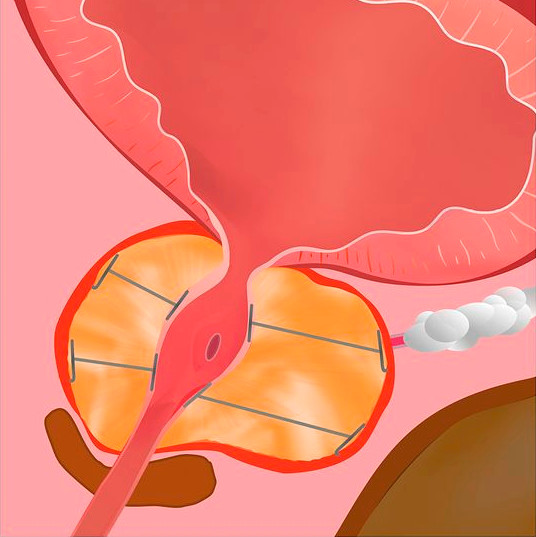
The prostate gland sits just below the bladder and covers part of the urethra. If it increases in size, it can put pressure on the bladder, urethra and bladder muscles. The urge then occurs much earlier than the bladder fills. Constant pressure can also weaken the bladder muscles, which means that the bladder does not empty completely and some urine remains in the bladder (so-called residual urine). At the same time, the pressure on the urethra prevents it from flowing freely.
A slow increase in the volume of the prostate gland is a normal process as the body ages. However, in some cases this increase is excessive. The reasons for this are not yet clear. A number of researchers attribute the condition to the onset of hormonal shifts in the body with age. Another assumption is the changing relationship between the individual structural elements of the organ with age.
In most cases, the complaints are mild or moderate and men adapt to them in everyday life. Sometimes there is even a temporary improvement in symptoms. But as a rule, they do worsen over the years, sometimes very slowly, sometimes quite quickly. And there often comes a point when it becomes clear that all this is very aggravating and requires active action.
Diagnosis
Benign enlargement of the prostate is the most common, but not the only possible cause of the above complaints. A specialized workup including a detailed anamnesis, urological clinical examinations (e.g. a digital rectal exam, urodynamic testing, etc.), a urological ultrasound scan, analysis of urine samples, certain blood parameters (e.g. PSA = prostate-specific antigen) is needed to make a diagnosis. In doubtful cases, the doctor will prescribe further diagnostic routine (e.g. radiologic studies).
Once the diagnosis of benign prostatic hyperplasia has been made, further monitoring and possibly treatment strategy will be determined.
BPH Stages
Doctors distinguish several stages of the disease development, which are important in terms of treatment choice.
| Stage I |
higher urination frequency and urination disorders, frequent nocturnal urge without residual urine. |
| Stage II |
residual urine exceeding 50 ml, with signs of decompensation (abnormal function). |
| Stage III | presence of complications. |
Possible consequences and complications
In addition to affecting a man's daily and, sometimes, also professional life, this condition can lead to serious health issues, such as:
- recurrent urinary tract infections;
- formation of bladder stones due to the presence of residual urine;
- urinary bladder neck varicosis and resulting hematuria;
- bladder muscle changes leading to urine flow into the ureters (reflux);
- reflux-related kidney damage, up to the development of renal failure;
- acute urinary retention requiring emergency measures with catheter placement and subsequent surgery.
BHP treatment approaches
Prostate adenoma can be quite burdensome, but in most cases is harmless.
Treatment strategy choice can usually be done without great haste.
Before taking action, one can think everything over calmly and get detailed information about the advantages and disadvantages of all available options. This is especially advisable if surgical treatment is proposed, as surgical intervention can also be associated with complications, sometimes very long-term ones.
Therapy
Your treating physician’s management strategy suggestions will depend on a variety of circumstances. The decisive factor is the patient's own assessment of how much the current complaints complicate their daily life, and the presence of complications (e.g. frequent urinary tract infections).
Besides, the treatment options likely to be applicable in a particular case are carefully weighed and their potential advantages and possible disadvantages are assessed.
Current treatment guidelines for this condition are based on the stage of the disease and the patient's subjective sensations.
In Stage I, it is usually sufficient:
- to monitor the condition without taking active measures; with mild symptoms and absence of complications, a check-up examination once a year is sufficient. Up to 30% of men diagnosed with benign prostatic hyperplasia do not need other medical procedures up to a certain point.
- to use plant-based remedies (phytotherapy): there are quite a few plant substances that can ease the symptoms of BPH. But the majority of them have not been studied well enough. The most common are preparations based on pumpkin and serenoa (dwarf palm). A doctor consultation is a must before starting such treatment; if there are doubts, be sure to seek a second opinion.
In Stage II, about 70% of patients who come to the doctor with typical complaints are started on medication, and at the drugs administered at this point are stronger than herbal medicines.
- Medications that relax the muscles of the prostate and bladder and facilitate urination (e.g. tamsulosin) are prescribed. However, these can also have a number of side effects such as dizziness, decreased blood pressure, etc.
- Drugs from another currently used group (e.g. finasteride) reduce the volume of the prostate by interfering with its hormonal metabolism, but have very little effect on symptoms.
- Volume reduction can also be achieved with anti-hormonal treatment (anti-androgens), but these quickly lead to impotence.
In stage III, or even earlier, disturbing symptoms may indicate the necessity of surgery even in the absence of serious complications.
Surgical treatment involves removal or destruction of prostate tissue with the help of various surgical techniques.
The most common method of surgical treatment of BPH nowadays is transurethral (i.e. with access through the urethra) surgery. Depending on the size of the organ, either transurethral incision (TUIP) or transurethral resection with an electric loop (TURP) is considered. This technique has proven to be highly effective and has become almost routine in many major urology centers.
If the prostate is too large, an open-surgical excision method with various access options is used.
The most common side effect of these surgeries is ejaculation disorder. Less commonly, erectile dysfunction or incontinence may occur.
Another complication is associated with the large amount of irrigation fluid getting into the vascular system and a marked decrease in sodium levels (TUR - syndrome).
These facts have inspired urologists to search for and develop alternative, minimally invasive, i.e. minimally traumatic methods of eliminating prostatic hyperplasia with fewer complications.
A review of current alternatives to surgical resection of prostate adenoma
In recent years, many urology hospitals in Europe and the United States have been increasingly adopting innovative technologies that help avoid some of the unpleasant consequences of conventional surgery.

The nitinol stent (i-TIND) is a self-expanding device consisting of three interwoven wire struts (nitinol is an alloy of nickel and titanium). It is inserted into the prostate bed under local anesthesia or short-time intravenous anesthesia. In 5-7 days after the procedure, three ducts are formed and the bladder neck is dilated, which leads to a significant improvement in urination, disappearance or relief of symptoms. This method has no significant side effects. However, it does not lead to the resumption of previously lost sexual function.
The urethral lift (UroLift®) ensures non-traumatic widening of the lumen of the urethra. This method has proven to be the most effective in preserving sexual function. Side effects are usually minor and short-term. But relatively often (11-13%), a repeat intervention is required after a few years. Currently, UroLift® is most recommended to patients for whom maintaining sexual function is a priority.

Vapor ablation (Rezūm™) is the reduction of prostate tissue volume using hot water vapor. It is delivered through a thin needle inserted into the prostate tissue in controlled amounts, with a very thin plastic tube (disposable endoscope) with a built-in camera first inserted into the urethra to monitor the procedure. Exposure to steam causes immediate prostate tissue cell death. As a result, the damaged tissue disintegrates within about three months, and the prostate shrinks. The procedure usually involves a bladder catheter placed for a short time.

Aquablation (AquaBeam®), a robotic waterjet procedure, is an innovative urological technique. It consists in the following: using a robotic system under real-time ultrasound image guidance, the prostate transition zone tissue is removed with a high-pressure saline jet. Like TURP, the procedure requires spinal or general anesthesia. This method is also similar to transurethral resection in terms of hospital stay duration, postoperative care, and recovery time. But aquablation is the only prostate resection procedure that offers a relatively high likelihood of maintaining sexual function. Among the risks of postoperative complications, bleeding is the most frequently mentioned.

Prostate artery embolization (PAE) is another modern way to treat prostate adenoma. It is a painless procedure that is performed under local anesthesia and x-ray guidance. The arteries of the prostate gland are probed with a microcatheter and sealed with microspheres. Lack of blood circulation in the corresponding area leads to tissue necrosis with secondary reduction in prostate volume. Accordingly, urologic symptoms disappear or are significantly reduced thereafter.
On the contrary, the larger the gland, the better the treatment works. But for now, it is considered experimental and should only be performed as part of clinical trials in appropriate urology centers. Sufficient data on the effectiveness of this treatment method has not yet been accumulated.

Transurethral microwave therapy (TUMT) involves heating overgrown prostate tissue and destroying it with low-energy microwaves. The destroyed tissue is either absorbed by the body itself or is excreted with urine. This treatment method also has a high-energy microwave option.
The table below summarizes the brief characteristics of different minimally invasive therapies for BPH (Data from Prof. Dr. Dr. Oliver Dudeck, M.D.). Oliver Dudeck, Centre for Microtherapy, Klinikum Hirslanden, Switzerland):
| Method | Working mechanism | Efficacy (symptom relief as measured by the IPSS*) | Advantages / Disadvantages |
|---|---|---|---|
| Nitinol stent (i-TIND) | Mechanic | by 9,2 points |
|
| Urethral lift (UroLift®) | Mechanic | by 9,9 points |
|
|
Vapor ablation (Rezūm™) |
Heating resulting in necrosis and volume reduction |
by11,6 points |
|
|
Aquablation (AquaBeam®) |
Water jet | by 14,4 points |
|
| Prostate artery embolization (PAE) | Transarterial embolization resulting in necrosis and volume reduction | By 9,2-21,0 points |
|
| *Internation Prostate Symptom Score |
To make the right choice, seek advice from a competent professional
All of the described innovative minimally invasive benign prostatic hyperplasia treatment methods relieve patient complaints as well as objective manifestations of the disease. Their advantages as compared to surgical resection include lower injury rates and complication risks, especially those related to sexual function. Nevertheless, the "pro" of TURP compared to sparing techniques is the significantly lower probability that a repeated procedure will be required.
Each of these methods has its own range of indications, depending primarily on the degree and localization of prostate tissue overgrowth.
Thus, the decision should always be customized, taking into account all relevant individual circumstances. The choice should be based on the opinion of a specialist with the appropriate knowledge and expertise in the application of all existing prostate adenoma treatment options, both conventional and innovative.
If there are no sufficiently competent urology facilities at your place of residence, you may benefit from a remote consultation possible by an overseas expert, which will provide answers to your questions regarding the best treatment options.
References:
- J. N. Cornu, S. Ahyai, A. Bachmann, J. de la Rosette, P. Gilling, C. Gratzke, K. McVary, G. Novara, H. Woo, S. Madersbacher: A Systematic Review and Meta-analysis of Functional Outcomes and Complications Following Transurethral Procedures for Lower Urinary Tract Symptoms Resulting from Benign Prostatic Obstruction: An Update. In: European urology. Band 67, Nummer 6, Juni 2015
- New medical device treats urinary symptoms related to enlarged prostate. Englisch. Pressemeldung der U.S.Food and Drug Administration vom 13. September 2013. Online auf fda.gov, abgerufen am 20. September 2013.
- BPH-6: Comparison of the UroLift System to TURP for Benign Prostatic Hyperplasia. Englisch. Online auf clinicaltrials.gov vom 6. Mai 2013
- H. Pham, P. Sharma: Emerging, newly-approved treatments for lower urinary tract symptoms secondary to benign prostatic hypertrophy. In: Can J Urol. Band 25, Nr. 2, 2018
- H. Saadat, D. S. Elterman: The Role of Aquablation for the Surgical Treatment of LUTS/BPH. In: Curr Urol Rep. Band 20, Nr. 8, 2019
- K. T. McVary, T. Rogers, C. G. Roehrborn: Rezūm Water Vapor Thermal Therapy for Lower Urinary Tract Symptoms Associated With Benign Prostatic Hyperplasia: 4-Year Results From Randomized Controlled Study. In: Urology, Band 126, 04 2019
Comments — 2
Александр
Кратко, лаконично и объективно.. Спасибо
Григорий
Прекрасная информация.спасибо.