

An atrial septal defect is a congenital abnormality. It is caused by the presence of an abnormal opening between the right and left heart chambers. Depending on the severity of the defect, it may not manifest itself at all, or may cause dyspnea, heart murmurs and other symptoms.
Surgery is the only way to treat an atrial septal defect (ASD). The technique is chosen depending on an individual situation.
What's an ASD
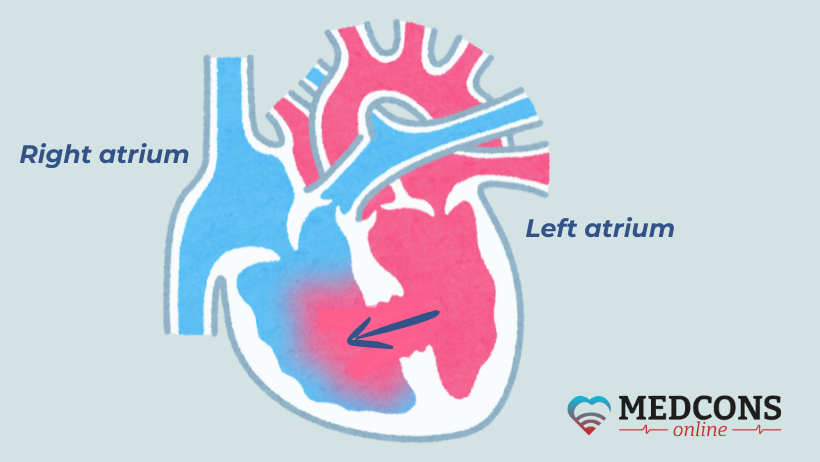
An atrial septal defect is one or more holes in the septum between the right and left atria. They cause abnormal discharge of blood, resulting in impaired haemodynamics.
ASD accounts for 5-15% of all congenital heart defects. In newborn girls, it occurs twice as often as in boys. It can be a single disorder, or may occur together with other congenital heart issues.
According to the defect location in the septum, three main types are distinguished:
Ostium secundum. In this case, the abnormal hole is located in the oval fossa, in the center of the interatrial septum.
Sinus venosus. The defect is found along the posterior wall of the septum, closer to the inferior or superior vena cava.
Ostium primum. The hole is located on the anterior side of the septum.
Symptoms depend on the type of defect.
ASD causes
In addition to the above, the abnormality may be provoked by:
- diabetes mellitus;
- endocrine disorders;
- long-time use of medications;
- alcohol consumption during pregnancy;
- exposure to radiation;
- complications of pregnancy.
What are the dangers of an ASD?
The condition may be complicated by infective endocarditis, while this complication is more common in other congenital heart defects. According to statistics, rheumatism develops in 10% of cases.
Haemodynamic features
The blood pressure in the left atrium is not the same as in the right. If there is a hole in the septum, an arteriovenous shunt occurs. The discharge volume depends on the size of the defect. As a result, the pulmonary circulation receives too much blood, and the load on the right atrium increases. At the same time, the right ventricle has to work too hard. Since the blood ejection volume does not match the size of the valve orifice, relative pulmonary artery stenosis develops.
After a certain period of time, the pulmonary hypervolemia provokes the development of pulmonary hypertension. This complication is more common in children over 15 years of age. In severe hypertension, right ventricular failure occurs.
Symptoms of atrial septal defect
An ASD can for a long time be accompanied by haemodynamic compensation. The severity of symptoms depends on the defect location and size, on how long the condition lasts, and the presence of complications.
If the defect was not detected in childhood, or a decision was made to monitor the condition without surgery, the child grows up without experiencing any health problems. In an adult, it is possible that the heart rhythm may be disturbed, especially after an illness.
Due to hemodynamic disturbance, the risk of clot formation increases, which can cause a heart attack or a stroke.
Manifestations of ASD in newborns
The only sign of the defect in the first month of life can be cyanosis that occurs during crying or restlessness. For this reason, such children are often diagnosed with perinatal encephalopathy.
If the defect is medium to large in size, the first signs of disorder appear in 3-4 months and include very pale skin, tachycardia, insufficient weight gain. Affected children often suffer from respiratory diseases accompanied by a long-lasting wet cough. The pulmonary circle hypervolemia is manifested by dyspnoe and dizziness. In older children, excessive fatigue and shortness of breath on exertion occur.
ASD diagnosis
ASD-specific examinations are aimed at determining the location and size of the opening. Also, in order to choose an effective treatment, it is important to determine:
- the volume of blood discharge;
- the presence or absence of pulmonary hypertension;
- the presence of arrhythmia;
- the presence or absence of concomitant defects.
First of all, echocardiography is necessary. The exam is absolutely safe for the patient and can be done at any age without any contraindications. In children, a conventional echo is sufficient, but in adolescents with excess weight and adults, it may need to be performed through the esophagus (transesophageal echocardiography) to ensure a better assessment.
The study can detect a defect, determine its size and location, as well as evaluate the edge status. Based on the results obtained, the doctor decides on the type of procedure.
Additional diagnostic options
ECG does not provide comprehensive information about anatomical anomalies of the heart. The electrocardiogram may show signs of right heart hypertrophy, rhythm changes, and the His bundle branch block.
In addition, a heart catheter may be used as an additional examination method. The purpose of the procedure is to close the defect in a minimally invasive way.
In more rare cases, a chest X-ray is done. The image may show changes in the right atrium and ventricle size, increased pulmonary vascularity and a pulmonary artery deformity.
If there are doubts about the ASD diagnosis, one can seek a second opinion from experienced congenital heart defect specialists.
Treatment
The defect cannot be repaired with drugs. Small defects may heal on their own within 1-2 years after birth. Such cases do not require therapy.
Cases where no surgery is performed include:
- Patients with an asymptomatic course of the disease, i.e., having no complaints and clinical manifestations. In this situation, the condition can only be detected by auscultation.
- Terminal disease stages with severe pulmonary hypertension, when the shunt has turned venoarterial with improper blood circulation in both circles.
- Eisenmenger syndrome (a secondary for of pulmonary hypertension).
Endovascular procedures
Larger secondary defects do not heal on their own and require treatment. Doctors recommend closing them at an early stage. Today, the most advanced method of treatment is endovascular closure of the defect, or a catheter procedure. A special device in the form of an umbrella (occluder) is used to close the hole in the septum, thus eliminating the backflow of blood. With proper placement of the occluder, the disorder can be healed completely. Occluders are available in a great variety of types, which enables doctors to choose the best option for a particular patient, matching the size of the defect, its location and the patient's age.
The operation is performed without general anaesthesia (with the use of sedation), under EchoCG guidance. The patient can be discharged from the hospital in 2-3 days. The procedure is indicated if there are both primary and secondary atrial septal defects.
Within 5-6 months, the occluder gets covered with a layer of endothelium and grows in completely. The patient is considered healthy ever since.
This type of procedure is not performed with large defects or if there are concomitant conditions. In these situations, conventional surgery under general aneasthesia is indicated.
If there are doubts regarding the choice of the endovascular method, one can use advice from doctors at European clinics. In European heart centers, occlude closure is the safest procedure with a success rate of over 95%.
Surgical treatment
In largeer defects, open-heart surgery is indicated. The surgeon uses a so-called patch made of a small tissue flap to repair the hole. To prevent complications, it is important to prevent an abnormal drainage of the pulmonary veins (vessel shift into the right atrium) before the operation, making sure that they are properly connected to the left atrium.
The treatment is performed after careful preparation and examination, under general anaesthesia. The patch grows in within 4-12 months, depending on the size and location of the defect, and lasts for life. Until the healing process is complete, blood thinning medications are to be taken for six months.
After a few months, the size of the right atrium returns to normal, the ASD symptoms disappear, and patients can lead a normal life, including lifting weights. Some patients may experience palpitations and rhythm disturbances during the first few weeks, which can be managed with medications.
After the operation, cardiology follow-up is a must. During the first year, quarterly visits are necessary. Later the intervals increase. Upon full recovery, it is enough to visit your heart doctor once a year.
ASD prognosis
Patients with minor defects may not be aware of them until old age. In some children they can close on their own in the first five years of life, provided the opening was small or medium in size.
In large defects, the lifespan without treatment is about 35-40 years. Death may be caused by heart failure, arrhythmia, or severe pulmonary hypertension.
A second opinion
A second opinion is the opportunity to receive counselling from experienced doctors from European clinics. Consultations are available both online and in written form. To obtain a second opinion, it is sufficient to share available examination results and recommendations, if any.
If the disorder was detected, a second opinion may be required:
To decide if surgery is appropriate. Experienced doctors can provide an accurate assessment of the patient's condition and determine if the procedure is necessary.
To determine the timing of surgery. The ASD is a congenital abnormality and the correct timing of the surgical procedure depends on a large number of factors.
To choose the surgery type. Today, quite a few atrial septal defect repair methods are available, and, given the importance of the organ, the choice should be particularly careful. Therefore, at this stage, the opinion of another doctor will be of great value.
References
- Atrial Septal Defect, Elisa A Bradley, 2020.
- Patent foramen ovale and atrial septal defect, Ahmed Kheiwa, 2020.
- Primum atrial septal defect, A M Sadeghi, 1997.
- Current concept of transcatheter closure of atrial septal defect in adults, Teiji Akagi, 2015.
Comments — 0