
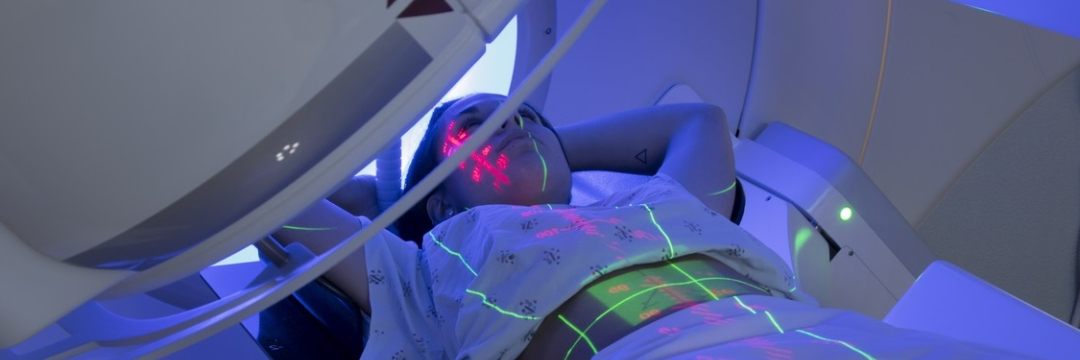
Along with surgery and various types of drugs, radiation therapy is an important component of combination treatment for malignant breast tumors. Its techniques and algorithms are being improved constantly in order to increase the effectiveness and safety of radiotherapy.
How does radiation affect breast cancer?
Ionizing radiation is capable of damaging the genetic material (DNA structure) of cells, both healthy and pathologically altered (malignant). However, for healthy cells such exposure is “habitual” because small amounts of X-rays constantly hit them, for example, from space. As a defense measure, they have developed a repair mechanism that works quite effectively up to a certain radiation dose limit. In cancer cells this limit is much lower than in normal ones, since their "repair system" is broken. Therefore, if the amount of radiation is properly divided into portions (the technical term is fractionated), it can be successfully used to treat cancer. The impact becomes destructive only for tumor tissues. This is what the use of radiation therapy in many cancers is based on, including breast carcinoma.
When should I get radiation therapy for breast cancer?
Radiotherapy is usually combined with surgical removal of the tumor. Today, the generally accepted standard is postoperative (adjuvant) radiation. Its special type is intraoperative radiation (IORT). However, in some cases radiotherapy is also used without surgery. In the case of advanced disease, it could be helpful in treating metastases.
Postoperative radiotherapy
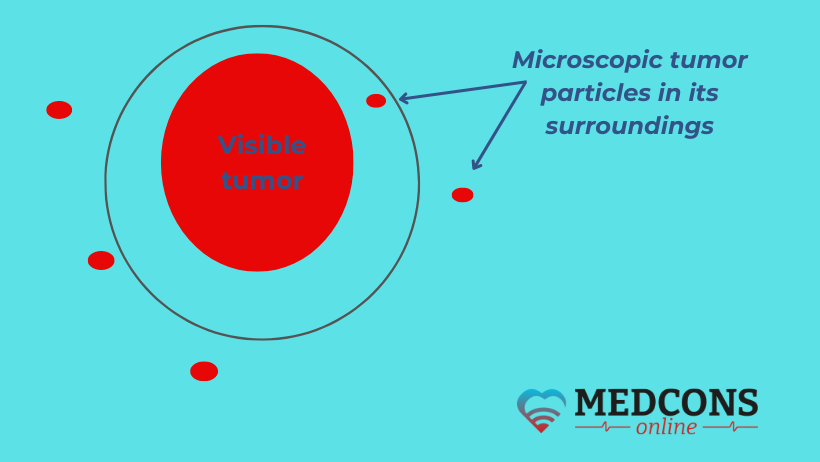
Malignant tumors spread imperceptibly, in the form of tiny particles, into the surrounding areas. This is why, for example, on microscopic examination, the abnormal mass is almost always larger than it appears to the naked eye. Thus, even if the tumor has been completely removed, small clusters of cancer cells may remain in the surrounding area. These microscopically small metastases are susceptible to X-rays, therefore radiotherapy is appropriate to prevent recurrence.
After organ-preserving resection of breast carcinoma, irradiation of all remaining glandular tissue has been recognized as an effective way to reduce the likelihood of disease recurrence, and is used almost all over the place. Cases where it can be abandoned are small-size, low aggressive tumors in the elderly without lymph node involvement.
After mastectomy, radiotherapy is required only in certain cases. It is mandatory for very large tumors that cannot be removed completely, if there is an increased risk of recurrence or if more than three lymph nodes are affected. If only 1-3 axillary lymph nodes are involved, and the tumor is of a low aggressive type, radiation to the chest wall can be avoided.
Radiation therapy without surgery
As an independent treatment method, it is only used if surgery is not possible (e.g. for inoperable tumors or with severe comorbidities), as well as surgery is refused.
IORT (intraoperative radiation therapy)
During the procedure, the site where the breast tumor used to be (the bed) is exposed to a single high dose of radiation during surgery, immediately after the mass has been removed. To do this, a balloon applicator is inserted into the resection field. A 50 kV X-ray beam is delivered through it, with the help of which a high dose is achieved both directly in the resection area and at a depth of several millimeters. Immediately behind the applicator, the beam intensity drops very sharply, so that only a quarter of it reaches a distance of 1 cm. This means sparing the surrounding tissue. After IORT, the applicator is removed and the operation is completed as planned.
This method has been shown to be effective as a substitute for the so-called "boost", i.e. additional radiation to the tumor bed to prevent recurrence. However, the procedure prolongs the duration of surgery. Therefore, for example, one of the leading German beast care experts, Ass. Prof.O. Glutz says:
Distant metastases
A fairly large proportion (> 50%) of breast carcinoma metastases involve the bones. Complications such as pathological fractures, pain, and spinal compression syndromes occur. Their treatment is multidisciplinary and, in addition to systemic drug therapy (cytostatics, antihormonal medications, targeted drugs) and palliative surgery, may include radiation. Its indications include:
- localized pain;
- restricted mobility,
- decreased bone stability (fracture risks),
- possible or existing neurological symptoms (e.g. spinal cord compression).
For multiple metastatic lesions, whole brain radiation is seen as the only option.
For liver metastases, radiation may be used in the form of SBRT (stereotactic body radiotherapy) or SIRT (selective internal radiotherapy), and stereotaxis is also used for secondary foci in the lungs. Radiation can also treat skin metastases.
Timing and combination with other therapies
Adjuvant radiotherapy for breast cancer should be started as soon as possible following surgery, immediately after the healing of postoperative wounds. The period between the 4th and 8th week after surgery is considered the best.
If chemotherapy is also recommended, radiation is usually given after the cytostatics to avoid more severe side effects.
Antihormonal therapy, antibodies as well as immunotherapy drugs, CDK4/6 inhibitors or capecitabine may be used alongside with irradiation.
Radiation therapy and breast reconstruction
Exposure to radiation can change the appearance of a breast that has been reconstructed either with tissue grafting or implants. Although the material of a modern implant does not get affected, the skin over it (or an autologous tissue flap) becomes denser, stiffer and inelastic. In addition, the risk of capsular contracture (thickening of the tissue around the implant) increases. Radiation also slows wound healing, which may lead to the development of infections.
Therefore, most surgeons recommend postponing reconstructive procedures in breast carcinoma until after radiation therapy.
Duration and dose of exposure
The duration and intensity of radiotherapy depends on the individual situation. The standard schedule is five days a week, one session per day, on an outpatient basis. Depending on the chosen plan, the course lasts from three to five weeks.
Modern clinical guidelines accept two breast cancer radiation modalities:
- Hypofractionated treatment (a total dose of about 40 Gy in 15-16 fractions delivered within about 3-5 weeks).
- Conventional fractionation (a total dose of about 50 Gy in 25-28 fractions over about 5-6 weeks).
If used as palliative treatment to relieve symptoms or control metastases, the course of radiotherapy can be significantly shorter.
Extra dose (boost)
Numerous studies have proven that booster radiotherapy ("supplementing" the total dose by high-intensity single-zone treatment) reduces breast cancer recurrence rates in all age groups, and is more effective in younger patients than in older ones. Therefore, professional associations strongly recommend adjuvant radiotherapy to all patients aged 50 years and younger, as well as to patients over 50 years if there is an increased risk of recurrence or histological risk factors.
Should the lymph nodes get exposed to radiation?
Until recently, radiotherapy to lymph nodes was considered appropriate only in rare cases, such as when several nodes in the axilla were affected. In recent years, however, this opinion has changed. The results of new studies show that radiotherapy may be more beneficial than surgical resection of lymph nodes in certain situations. Therefore, lymph node exposure is increasingly frequent, and is expected to be so in the future.
What types of radiation are used for breast cancer?
The standard procedure is external beam radiation using a linear accelerator, which is delivered through the skin; more than 95% of all patients worldwide are treated in this way. Today, modern technology allows very precise control of the process, achieving a high concentration of radiation only in the desired area (the cancerous lesion) without damaging the surrounding healthy tissue. For this purpose, devices that emit radiation from different directions are used, and only the cells in the area where the rays intersect are damaged.
Brachytherapy (brachy = Greek for "short, close") can be used as an alternative to external radiation. In this procedure, also known as "internal radiotherapy", a radioactive substance is delivered directly into the bed through small plastic catheters under a short general anaesthetic. These catheters are inserted during breast surgery and remain in place for the duration of treatment. The course lasts from 1 to 5 days.
Side effects
Any treatment is associated with risks. But thanks to various technical improvements, radiotherapy today is much more precise and much better tolerated than it used to be.
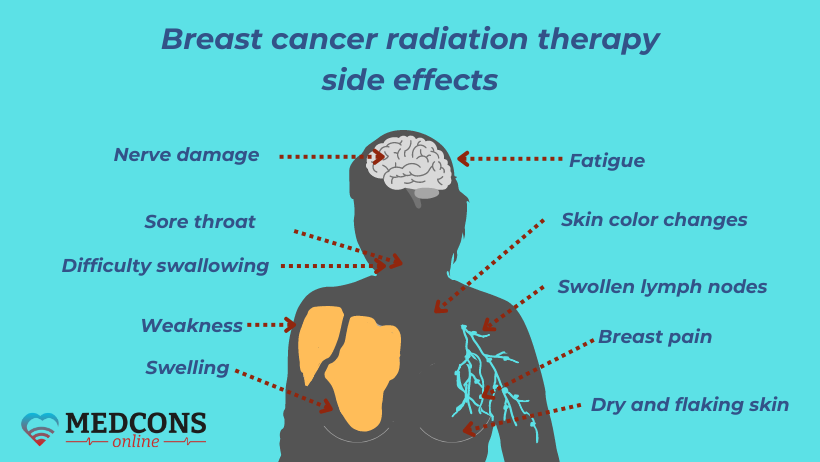
Only the breast tumor is the aim, while the neighbouring organs are hardly affected. Nevertheless, breast exposure to external radiation is a stressful experience, especially for the skin in the affected area. The consequences can be similar to those of a severe sunburn: painful redness and even blisters, as well as hair loss.
A reaction in the form of nausea and vomiting is also possible. The frequency and severity of these unwanted side effects depend on the dose, site and type of radiotherapy. In general, however, nausea is less frequent with radiotherapy than with chemotherapy. Also, there are effective drugs that can suppress it; an adapted diet may also help.
If the area of radiation exposure includes lymph nodes, there is a possibility of lymph stasis (lymphoedema) in the chest or arm.
Central nervous system disorders, sore throat and difficulty swallowing, breast pain and fatigue are likely, although far less common.
Technical innovations
Advanced clinics and radiation oncology departments use state-of-the-art techniques to deliver breast cancer radiation therapy with minimal side effects.
Intensity modulation (known as IMRT, or Intensity-modulated radiotherapy) ensures reliable protection of organs or body tissues near the tumor, that are particularly sensitive to radiation. In addition, it is possible to vary the intensity of exposure to different areas of the mass. In this way, the dose can be best adapted to lesions with complex shape. A sufficient dose can be applied to tumors in close proximity to high-risk organs without damaging healthy tissue.
VMAT (Volumetric Intensity Modulated Arc Therapy) is a further development of IMRT technology. In this case, an radiation device rotates around the patient, which allows for constant adjustment of both the field shape and the radiation intensity.
The high-energy ("fast") electrons obtained thanks to acceleration technology produce ultra-hard X-rays that can be focused as much as possible with minimal exposure time.
Visual control in IGRT (Image-guided radiation therapy) is achieved with a special CT scanner integrated into the linear accelerator. It helps to correct the current position of the patient during the session by comparing it with the CT data obtained during pre-planning. In this way, the treatment becomes even more targeted.
The Deep Inspiration Breath Hold (DIBH) technique makes it possible to limit the radiation load on the heart and lungs in the case of left breast cancer.
What is the procedure for external beam breast radiation?
Radiotherapy is performed on an outpatient basis, is non-invasive (and therefore does not require anaesthesia) and is therefore easily incorporated into everyday personal and professional life. For breast cancer, external radiation is fractionated. This means that the total dose is divided into several daily parts (fractions) and the treatment is given over a period of 3-4 weeks.
Preliminary appointment
Before the course starts, there is a detailed initial consultation with a radiation therapist, during which the specialist studies the anamnesis, medical reports and imaging diagnostics (mammography, sonography, CT or MRI). The treatment procedure is also discussed in detail at this point.
CT planning
For the preparation and planning of radiotherapy, a CT scan is performed. It provides precise information about the individual anatomy as well as the size and location of the tumor to be treated. The CT scanner is used to create body cross-sections every 1 to 3 mm. On each slice, the area to be treated ("target area") and organs requiring special protection are marked with millimetre precision.
Once the planning is done, marks are placed on the skin for more precise positioning. The CT scan data is transmitted to a computer, where a medical physicist works with a radiation oncologist to draw up an optimal radiation plan. The aim is to apply the highest possible dose without affecting the surrounding healthy tissue in order to minimize possible side effects.
First and following on sessions
It is on the first treatment day that the radiation fields are adjusted, so it is particularly important. The initial adjustment is carried out with the participation of radiological technicians. State-of-the-art visual inspection technology and CT scanners are used to check that the radiation fields conform to the prescribed parameters, allowing for a high-precision position check before radiotherapy begins. After position checking, the fields are marked on the patient's body and even the slightest deviations can be immediately detected and corrected during the next sessions.
During irradiation, the patient is positioned on the treatment table. The radiation source moves around at a distance of one meter. There is a constant visual and voice contact with the doctor through monitors and microphones. The duration of the first session is 30-40 minutes, other sessions take about 15 minutes. The treatment itself lasts only about two minutes, the rest of the time is taken up by initial adjustments and later on by positioning and controlling the device.
How should you behave and what should be watched out for
Objectively speaking, percutaneous radiotherapy is nowadays the least risky of all breast cancer treatments, including even hormone therapy. Recommendations to those who are going to get it are very simple. During the whole therapy course, it is recommended:
- to avoid wearing tight clothing that might irritate the exposed skin areas;
- not to use irritating skin care products;
- to avoid skin expose to strong heat (e.g. sunbathing or sauna);
- to use moisturising and cooling lotions;
- to cover the skin marks with a transparent patch when bathing or showering so that they do not get rubbed off.
Regular medications (such as those for hypertension or diabetes) should be continued without change. Patients with a pacemaker may need to get it checked regularly, with reprogramming if necessary.
How do I protect my skin during breast radiation therapy?
As radiotherapy itself is a strain on the skin, additional irritation should be avoided much as possible. It is therefore necessary to keep the affected skin areas clean and dry. Special care should be given to skin folds.
Everyday life tips:
Personal hygiene
- Use pH-neutral soap or shower gel for personal hygiene.
- Avoid perfume, deodorants and other fragrances.
- Minimize contact with water (do not take a bath, or swim).
- Lightly pat damp skin instead of rubbing it.
Skin protection
- Wear loose, lightweight clothing made of soft fabrics.
- Avoid direct sunlight.
- Avoid mechanical stress on the skin (massage, jewellery, band-aids).
- Avoid exposure to very hot or very cold temperatures.
During the treatment course, it is advisable to apply creams to the affected areas (avoiding the marks) twice a day and only after the session.
It is also advisable to use quality sunscreens with a high sun protection factor (>15), especially mineral-based. Sprays are the preferred form as they do not need to be rubbed in.
If redness and mild itching occur, soothing creams can help. They are applied in a thin layer to prevent heating.
There are special creams designed for irradiated skin, which are very easy spread due to their light consistency.
Home remedies such as sour cream compresses (without direct contact with the skin) can also help with mild redness and itching. However, if severe and painful skin reactions occur, a doctor should be consulted to take appropriate action.
What happens during internal radiotherapy for breast cancer?
Brachytherapy is done in hospital. At the first stage, thin (1.6 mm in diameter) plastic tubes (catheters) are inserted into the target area under anaesthesia and CT or X-ray quidance. The procedure takes about 15-20 minutes.
After the anaesthesia has worn off, a CT scan is performed to check the position of the catheters and provide for radiation planning. The next day, after the dose distribution has been calculated, the first brachytherapy session takes place. An iridium-192 gamma irradiator is inserted into the plastic catheters under remote CT control. Only the target areas are exposed. The treatment is administered twice a day (morning and afternoon), 8 times in total, each session taking about 15 minutes. The treatment is not accompanied by any unpleasant sensations, no anaesthesia is required.
After the last radiotherapy session, the catheters are removed and patients are discharged from hospital the next day.
In particular, radiation effects on the heart, lungs and finally the skin are minimal. Catheter placement is a short and minimally invasive procedure that is usually well tolerated and has no unpleasant consequences.
After some time, hardening/rubbing may be felt in the area of the tumor bed due to both breast surgery and internal radiation, but in most cases these are not bothersome.
What should I do if I am to get radiotherapy for my breast cancer?
First of all, do not get frightened. Despite the fact that the word "radiation" is quite reasonably associated with danger to life, it should be remembered that in this case it will be targeted not at the whole body, but at the "evil" that has settled in it and must be eradicated. A whole team of professionals (radiologists, medical physicists, technicians) will work hard to defeat the malignant process without harm to healthy tissues and organs, using carefully developed technologies and high-tech equipment.
If your doctor refers you for radiotherapy, do not hesitate to ask questions to clarify for yourself all the points related to the upcoming treatment. This will help you better understand its essence, goals and objectives, relieve understandable anxiety and fear of the unknown.
Do not succumb to pessimistic moods that may arise from reading entries in thematic Internet forums. People tend to "spill" into the network their negative emotions and experiences, behind which the positive side, i.e. the result, may remain "in the shadows". Objective information is to be found in a professional environment, including second opinions.
How can a radiotherapy second opinion help in breast carcinoma?
The indications for radiotherapy in malignant breast diseases and the possible options for its use in certain clinical situations are generally standardized and described quite clearly in professional guidelines.One might ask, what does the second opinion have to do with it?
However, this particular malignant disease is special.
Physicians are challenged with a difficult task, including a comprehensive assessment of the specifics of a particular case, decision whether radiation exposure is really necessary and choosing the best treatment plan. It is important that in decision-making, the specialist does not blindly follow the standards, but is able to flexibly adapt the available arsenal of options to the individual situation, maintaining an optimal balance between potential benefits and possible damage to health. Therefore, seeking another opinion on breast cancer radiotherapy is quite reasonable, especially if the expert is an internationally recognized specialist. In this way, with the help of the experience of world medicine and its most current achievements, one can improve the existing recommendations or make sure once and for all that they are indeed correct.
The key question is which specialist should be contacted for such counselling. The answer varies from country to country. In Germany, for example, on issues concerning breast cancer radiation therapy, one can seek a breast care expert second opinion. Of course, the treatment itself primarily involves professionals from fields such as radiology, mathematics and physics. Still, it is a breast care specialist who makes major decisions. Our MedconsOnline service cooperates with the best doctors who will thoroughly understand all the nuances of your problem and help you find solutions based on advanced knowledge and solid clinical experience.
References
- Hennequin C, Belkacémi Y, Bourgier C, Cowen D, Cutuli B, Fourquet A, Hannoun-Lévi JM, Pasquier D, Racadot S, Rivera S. Radiotherapy of breast cancer. Cancer Radiother. 2022 Feb-Apr;26(1-2):221-230. doi: 10.1016/j.canrad.2021.11.013. Epub 2021 Dec 23. PMID: 34955414.
- Bauer A. Radiation Treatment for Breast Cancer. Surg Clin North Am. 2023 Feb;103(1):187-199. doi: 10.1016/j.suc.2022.08.015. Epub 2022 Oct 17. PMID: 36410350.
- Dunst J, Krug D. Boost und Hypofraktionierung beim DCIS [Boost and hypofractionation in DCIS]. Strahlenther Onkol. 2022 Dec;198(12):1122-1124. German. doi: 10.1007/s00066-022-02016-y. Epub 2022 Oct 20. PMID: 36264356; PMCID: PMC9700622.
- Sperk E. Bestrahlen oder nicht bestrahlen bei älteren Patientinnen mit Low-Risk-Mammakarzinom? Erkenntnisse aus den 10-Jahres-Daten der PRIME-II-Studie [To irradiate or not to irradiate low-risk breast cancer in older women? Insights from the 10-year data of the PRIME II trial]. Strahlenther Onkol. 2023 May;199(5):520-521. German. doi: 10.1007/s00066-023-02071-z. Epub 2023 Mar 27. PMID: 36971810; PMCID: PMC10133080.
Comments — 0